Yesterday I took the Comprehensive Basic Science Exam (CBSE). This is an exam covering the first two years of medical school that is put out by the National Board of Medical Examiners (NBME). They're the same people who write and administer the medical boards. There were four sections (Step 1 has seven sections), each with fifty questions, and we had a total of four hours to complete the exam. The questions cover everything from first and second year, with a heavier emphasis on second year subjects like pathology and pharm. Suffice it to say that the test was really hard, especially since we haven't covered half the material yet! I would say in each section there were about 25% questions that I knew, 50% of questions where I could eliminate the answers down to two or three choices, and 25% where I had absolutely no clue whatsoever. The good part is that I had no trouble finishing in time. In fact, I went through the entire test three times and was still finished 45 minutes early.
It's unbelievable how fast the time has gone by. I'm now officially halfway through my second year of medical school. We finished the diabetes PBL case, and we had two seminars today, one on hypoglycemia and one on the complications of diabetes. They were both pretty good. The first seminar leader asked me to pretend to have hypoglycemia, so I was shaking, sweating, having a headache, and then I "fainted." After we talked about the symptoms of hypoglycemia, she gave me a little bag of Skittles. I guess that is supposed to be a glucose source to take care of my "hypoglycemia." The second seminar leader is the same endocrinologist that I had endocrine clinic with last week. It was funny, because he remembered me, but he clearly didn't remember my name and he didn't want to have to ask me what it was again.
In the afternoon, I did some errands and went to the gym. I don't normally go to the gym on Fridays, but they are closing all weekend for Christmas, so I can't go tomorrow like I usually do. Then I wrote evals for my PBL group and cleaned the lounge refrigerator and microwave. We have a signup sheet to clean out the fridge every couple of weeks, so that wasn't too bad. But the micro was absolutely disgusting. I don't know when it was cleaned last, but it probably was years ago.
Grades for my MS classes came out today from Case: two As in epidemiology and clinical trials, and a B in biostatistics. I was expecting the clinical trials and stats grades, but the A in epi came as a pleasant surprise. Looking back over the past year, I realize that although having to do the extra work for the MS was miserable sometimes, overall I'm glad that I stuck it out. It's one of those things that isn't always fun while you're going through it, but the short-term pain is worth the long-term gain. I guess that is true of medical school in general.
We have SAQs and CAPPs to do over break like normal. I am planning to do them this weekend and get them over with by Monday morning at the latest. I also have clinical homework to do for my first week back in January, which involves preparing patient presentations for my FCM group and my clinical reasoning group. The clinical reasoning class is something new, and we are doing that instead of longitudinal clinic the first week. I just realized that I will be doing BOTH presentations on Tuesday of my first week back. Well, at least I'll get it all over with early. It looks like we go back to clinic as usual after that first week.
I want to wish all of my blog readers a Merry Christmas and a Happy New Year. I'll see you all next year. :-)
Friday, December 21, 2007
Wednesday, December 19, 2007
Double Communications
Our PBL patient is not doing so well. This case has turned out to be a lot more interesting than we had expected, because we had a diabetes PBL case last year too. But this one focuses more on the long term complications for patients who do not have controlled diabetes. Unfortunately, the truism that being an interesting patient is a bad thing definitely holds true here. The seminars were on gestational diabetes (pregnant women become insulin resistant and can even become diabetic while pregnant) and nutrition.
This afternoon we had double communications for four straight hours, which would ordinarily have been fairly painful. But, one of my group members didn't show up at all and another didn't get a chance to video an interview with a patient, so we actually got out about an hour and a half early. The first part of the session was about how to deal with family members being in the room. I got a mother-teenage daughter duo where the mother kept trying to take control of the interview. These were standardized patients, and the two actors I had were terrific. I would have totally believed that they were a mother and daughter for real. I was able to tone the mom down a little by turning my chair so that my side was to her and I was directly facing the daughter. I even managed to get her to leave the room, though she really didn't want to, and at that point I stopped. I could have kept going and done a sexual history on the daughter at that point, but I figured we've already done that lesson, and I'd gone on long enough.
The video reviews took another hour. I had been counseling my patient (a real one this time, the same interview that I taped last week) about smoking cessation, and I could have definitely gone further with that. When we got done, there were big, fat snowflakes falling outside. It was beautiful to watch, though what it did to the afternoon traffic was not at all beautiful. We haven't been getting too much snow yet this winter, but today is more than making up for that.
This afternoon we had double communications for four straight hours, which would ordinarily have been fairly painful. But, one of my group members didn't show up at all and another didn't get a chance to video an interview with a patient, so we actually got out about an hour and a half early. The first part of the session was about how to deal with family members being in the room. I got a mother-teenage daughter duo where the mother kept trying to take control of the interview. These were standardized patients, and the two actors I had were terrific. I would have totally believed that they were a mother and daughter for real. I was able to tone the mom down a little by turning my chair so that my side was to her and I was directly facing the daughter. I even managed to get her to leave the room, though she really didn't want to, and at that point I stopped. I could have kept going and done a sexual history on the daughter at that point, but I figured we've already done that lesson, and I'd gone on long enough.
The video reviews took another hour. I had been counseling my patient (a real one this time, the same interview that I taped last week) about smoking cessation, and I could have definitely gone further with that. When we got done, there were big, fat snowflakes falling outside. It was beautiful to watch, though what it did to the afternoon traffic was not at all beautiful. We haven't been getting too much snow yet this winter, but today is more than making up for that.
Tuesday, December 18, 2007
Clinic Christmas Party
This week we are covering diabetes in excruciating detail. All four seminars from yesterday and today were about diabetes, and our PBL case is about the long-term complications of diabetes. So, it was only fitting that today was my clinic's annual office Christmas party. I got off easy with just bringing jello. Other people baked brownies, made homemade mashed potatoes, and someone even brought fried chicken. Oh, and I shouldn't forget about the macaroni and cheese. All of which, while completely delicious, are exactly the types of diabetogenic foods that are going to ensure that many of us partygoers will be the future diabetic and coronary artery disease patients who keep the Cleveland Clinic prospering for the next several decades.
The other nice thing about today is that I got about an hour and a half off between seminar this morning and the office party, so I got through with most of tomorrow's reading. Our FCM class today consisted of each of us meeting with the small group preceptor for about ten minutes. I got to go right at 10:00 as soon as the second seminar was over. Since my group's preceptor has been gone the last few weeks, I almost blew the meeting off altogether. But I decided I should probably stop by to see if he was there, and it's a good thing I did, because he did show up. These ten minute meetings are pretty pointless. They are supposed to be for us to get and receive feedback. But the feedback we get is useless because it's oral and can't be used for our portfolios. And giving too little feedback to the preceptor has never been a shortcoming of mine. He told me that I should try not to be so frustrated with the class. I wouldn't say I'm all that frustrated, but maybe I just expressed my feelings about these ten minute meetings a little more strongly than I intended. :-P
A few of our patients didn't show today, and the clinic was pretty quiet in general except that people kept coming by the break room to eat party leftovers. The nurses tried to get me to take some food home with me, but I didn't. I am sure the only reason I don't already weigh five thousand pounds is because I never bring any junk food home with me. That being said, I did manage to eat three brownies during the course of the afternoon.
The other nice thing about today is that I got about an hour and a half off between seminar this morning and the office party, so I got through with most of tomorrow's reading. Our FCM class today consisted of each of us meeting with the small group preceptor for about ten minutes. I got to go right at 10:00 as soon as the second seminar was over. Since my group's preceptor has been gone the last few weeks, I almost blew the meeting off altogether. But I decided I should probably stop by to see if he was there, and it's a good thing I did, because he did show up. These ten minute meetings are pretty pointless. They are supposed to be for us to get and receive feedback. But the feedback we get is useless because it's oral and can't be used for our portfolios. And giving too little feedback to the preceptor has never been a shortcoming of mine. He told me that I should try not to be so frustrated with the class. I wouldn't say I'm all that frustrated, but maybe I just expressed my feelings about these ten minute meetings a little more strongly than I intended. :-P
A few of our patients didn't show today, and the clinic was pretty quiet in general except that people kept coming by the break room to eat party leftovers. The nurses tried to get me to take some food home with me, but I didn't. I am sure the only reason I don't already weigh five thousand pounds is because I never bring any junk food home with me. That being said, I did manage to eat three brownies during the course of the afternoon.
Friday, December 14, 2007
Surviving My MS
Yesterday was kind of a hectic day, but I did get my paper done in time, and I gave my presentation for class. I got a few good suggestions as well as one softball question from someone who missed the first part where I explained the rationale. So that's it. I'm officially done with my second MS class. One more week to go until break!
Today's seminars were on thyroid disease and autoimmunity of the endocrine system. They were both good ones. The first one was taught by the doc who heads this block, and he's a really energetic and enthusiastic kind of guy. The second one was a really good review of the immunology we covered last spring, and it also specifically went into how the immune system interacts with the endocrine system.
For POD, we had the group presentations on the projects we came up with last week, and these were much smoother than the previous time we did this. Our group was the only one that came up with the stem cell idea, which is cool. Last time, it seemed like all four groups pretty much came up with the same project.
I am incredibly tired but oh so happy to be done with my MS class. It's not that any of it is hard. It's just a lot of work sometimes. On the good side, I registered for my courses for next semester today, and I just realized that I have basically finished the entire MS except for my advanced stats class and the research year/thesis. That's pretty incredible. No wonder I feel so tired. I basically did all of my MS coursework except one class in one year while being a full-time medical student! I could do the advanced stats class next semester, but I decided not to because I want to have some time to start studying pharm and micro before the final push to study for Step 1. This year is just going by so fast....
Today's seminars were on thyroid disease and autoimmunity of the endocrine system. They were both good ones. The first one was taught by the doc who heads this block, and he's a really energetic and enthusiastic kind of guy. The second one was a really good review of the immunology we covered last spring, and it also specifically went into how the immune system interacts with the endocrine system.
For POD, we had the group presentations on the projects we came up with last week, and these were much smoother than the previous time we did this. Our group was the only one that came up with the stem cell idea, which is cool. Last time, it seemed like all four groups pretty much came up with the same project.
I am incredibly tired but oh so happy to be done with my MS class. It's not that any of it is hard. It's just a lot of work sometimes. On the good side, I registered for my courses for next semester today, and I just realized that I have basically finished the entire MS except for my advanced stats class and the research year/thesis. That's pretty incredible. No wonder I feel so tired. I basically did all of my MS coursework except one class in one year while being a full-time medical student! I could do the advanced stats class next semester, but I decided not to because I want to have some time to start studying pharm and micro before the final push to study for Step 1. This year is just going by so fast....
Wednesday, December 12, 2007
Endocrine Clinic
It's fortunate that I got that book about women's health on Monday when I had the chance, because my learning objective for Friday is about hormone replacement therapy (HRT). There are two chapters in there describing all of the HRT drugs, and it is even readable and informative. The seminar today was about puberty disorders. That is some weird stuff. I hadn't realized though how young normal girls are when they begin puberty. I would have guessed about age 12, but that's just the average age when girls start menstruation. Girls begin developing breasts and pubic hair a couple of years earlier, around age 10.
This afternoon, I had endocrine clinic. My classmates who went yesterday were complaining that all they saw were diabetes patients. But today my classmate and I saw all thyroid patients, except for one infertility patient. I think this doc we were with must be a thyroid specialist. It was so busy in the clinic though that we really didn't get a chance to discuss anything with him much. Plus, there was also a fourth year med student working with him. So my classmate and I didn't wind up getting to do very much except for once when the doc had to leave the room to answer a page. That patient had hyperthyroidism and was willing to let my classmate and me both examine his thyroid. I couldn't really notice too much difference from a normal thyroid. Maybe it felt a little softer and slightly enlarged, I guess.
When it was time for us to go, the doc offered to let us stay on and keep following him and the fourth year student around, but my classmate and I had both seen enough for one day. The endocrine clinic was more interesting than I had expected it to be, but I was disappointed about how little we got to do compared to some of the other students in my class.
This afternoon, I had endocrine clinic. My classmates who went yesterday were complaining that all they saw were diabetes patients. But today my classmate and I saw all thyroid patients, except for one infertility patient. I think this doc we were with must be a thyroid specialist. It was so busy in the clinic though that we really didn't get a chance to discuss anything with him much. Plus, there was also a fourth year med student working with him. So my classmate and I didn't wind up getting to do very much except for once when the doc had to leave the room to answer a page. That patient had hyperthyroidism and was willing to let my classmate and me both examine his thyroid. I couldn't really notice too much difference from a normal thyroid. Maybe it felt a little softer and slightly enlarged, I guess.
When it was time for us to go, the doc offered to let us stay on and keep following him and the fourth year student around, but my classmate and I had both seen enough for one day. The endocrine clinic was more interesting than I had expected it to be, but I was disappointed about how little we got to do compared to some of the other students in my class.
Tuesday, December 11, 2007
Rants of a Crank
Our PBL case this week is about premature ovarian failure, and it's an interesting one so far. We had two seminars yesterday, one on deficiencies of adrenal enzymes and one on menopause, to go with it. The menopause seminar speaker has written a book on the topic, and she gave free copies to anyone who wanted one. Her powerpoint slides were disgustingly pink, the presentation made annoying little cutesy noises every time she changed slides, and her talk was half science and half soap box. But it's amazing how getting a free book can make all of these sins of powerpoint presentations forgivable.
In the evening, CCLCM was co-sponsoring an event at the Maltz Museum so that all the Case medical students could see the Deadly Medicine exhibit for free. It's the same exhibit that I went to a few months ago, only this time we didn't get to go to Mrs. Lerner's house afterward. Someone cancelled at the last minute, so there was an extra ticket, and I was able to go back to see the parts that I didn't make it to last time. I didn't stay too long though because I still had to do some more work on my paper for my MS class.
This morning, we had seminars on osteoporosis and thyroid pathology, and then for FCM we had a "field trip" to the art museum. I had been asked to participate in the NMS block evaluation session, scheduled for today at lunch. But I couldn't do it, because I had to videotape myself interviewing a patient in clinic. This is a ridiculous new requirement that all the first and second years have to do this year, where we check out a video camera, print out a consent form, and take them both to clinic to video an interview with a real patient. I wouldn't have minded as much if I could have scheduled the day myself, but the school decided to make me do it today, which is about the worst day they could have picked all block for me. They had also scheduled me to have a clinical correlation today, so I had to go see someone in administration to get it straightened out. I dare say that I'm a pretty decent multi-tasker, but even so, I readily confess that I'm not so good that I can be in two different clinics at the same time.
The actual patient interview taping went ok once I got everything set up. As it turns out, my first patient consented to be interviewed on tape, and he was some kind of video camera whiz, so he even set it all up for me. It was good that I did the videotaping early in the afternoon, because as usual we were double booked from 3-5 PM, and all four of those patients showed up today.
I was completely puzzled by one of my patients. She wanted to get pregnant but couldn't, so she was interested in infertility treatments. She said she'd been trying to get pregnant for several years. That definitely fits the definition of infertility, which is an inability to conceive after one year or more of trying. I asked her about the regularity of her menstrual cycles and age of menarche. Both were normal and she hadn't noticed any changes in her menstrual cycles. Did she take birth control? No. Was she using condoms? No, she was having regular, unprotected intercourse. Did she have a medical condition that could interfere with her fertility? None that either of us could think of. How about her husband? He didn't have any known infertility problems. At a complete loss, I started going through her medications on the computer, and what do you know, she had been getting intramuscular injections of Depo Provera for the past few years. At that point, I excused myself from the room and went to get my preceptor. I suppose I could have just told her myself. But I figure this is one of those things where it's better for the patient to hear it from the physician and not some second year medical student!
In the evening, CCLCM was co-sponsoring an event at the Maltz Museum so that all the Case medical students could see the Deadly Medicine exhibit for free. It's the same exhibit that I went to a few months ago, only this time we didn't get to go to Mrs. Lerner's house afterward. Someone cancelled at the last minute, so there was an extra ticket, and I was able to go back to see the parts that I didn't make it to last time. I didn't stay too long though because I still had to do some more work on my paper for my MS class.
This morning, we had seminars on osteoporosis and thyroid pathology, and then for FCM we had a "field trip" to the art museum. I had been asked to participate in the NMS block evaluation session, scheduled for today at lunch. But I couldn't do it, because I had to videotape myself interviewing a patient in clinic. This is a ridiculous new requirement that all the first and second years have to do this year, where we check out a video camera, print out a consent form, and take them both to clinic to video an interview with a real patient. I wouldn't have minded as much if I could have scheduled the day myself, but the school decided to make me do it today, which is about the worst day they could have picked all block for me. They had also scheduled me to have a clinical correlation today, so I had to go see someone in administration to get it straightened out. I dare say that I'm a pretty decent multi-tasker, but even so, I readily confess that I'm not so good that I can be in two different clinics at the same time.
The actual patient interview taping went ok once I got everything set up. As it turns out, my first patient consented to be interviewed on tape, and he was some kind of video camera whiz, so he even set it all up for me. It was good that I did the videotaping early in the afternoon, because as usual we were double booked from 3-5 PM, and all four of those patients showed up today.
I was completely puzzled by one of my patients. She wanted to get pregnant but couldn't, so she was interested in infertility treatments. She said she'd been trying to get pregnant for several years. That definitely fits the definition of infertility, which is an inability to conceive after one year or more of trying. I asked her about the regularity of her menstrual cycles and age of menarche. Both were normal and she hadn't noticed any changes in her menstrual cycles. Did she take birth control? No. Was she using condoms? No, she was having regular, unprotected intercourse. Did she have a medical condition that could interfere with her fertility? None that either of us could think of. How about her husband? He didn't have any known infertility problems. At a complete loss, I started going through her medications on the computer, and what do you know, she had been getting intramuscular injections of Depo Provera for the past few years. At that point, I excused myself from the room and went to get my preceptor. I suppose I could have just told her myself. But I figure this is one of those things where it's better for the patient to hear it from the physician and not some second year medical student!
Friday, December 07, 2007
A Day Devoted to Research
I had thought up until about a week ago that the final paper was due for my clinical trials class yesterday because I wrote it down wrong in my calendar, but I got a reprieve. It's not due until next week. So, I am going to be spending this weekend working on it, but I'm very, very grateful for the extra week! The other nice thing is that after next week, there will be no more crack of dawn Thursdays for me for the rest of this year.
Today we finished our PBL case and had two seminars on pancreatic tumors and ectopic hormone production. ("Ectopic" means that the hormone is being produced by tissue somewhere in the body that isn't supposed to be producing it.) We also had another one of those small group research planning sessions instead of the normal POD/ARM seminar. I was initially wary after how badly the last one went, but this one was a lot better. A big part of it is that our PBL case this week had several engaging scientific and ethical issues (unlike the last one we had to use), and we came up with a research idea that is actually interesting. I'm not sure how feasible it is, but it would be cool if it could be done. Basically, we want to look at pancreatic tumor markers to differentiate tumors which secrete hormones that are normally produced by the pancreas (ex. insulin) versus tumors which secrete hormones not usually produced by the pancreas (ex. growth hormone). Our hypothesis is that the former come from differentiated pancreatic cells, while the latter come from from pancreatic stem cells. The existence of pancreatic stem cells was only discovered quite recently, so it's a hot field.
This afternoon, I met with a researcher who I am considering working with for my research year. We discussed some possible ideas. I wasn't particularly gung ho about any of them, but he was open to me coming up with something else. So I really need to spend some time thinking about exactly what project I want to work on this spring and summer. Then I will need to start working on convincing someone to fund me for it. :-P
Today we finished our PBL case and had two seminars on pancreatic tumors and ectopic hormone production. ("Ectopic" means that the hormone is being produced by tissue somewhere in the body that isn't supposed to be producing it.) We also had another one of those small group research planning sessions instead of the normal POD/ARM seminar. I was initially wary after how badly the last one went, but this one was a lot better. A big part of it is that our PBL case this week had several engaging scientific and ethical issues (unlike the last one we had to use), and we came up with a research idea that is actually interesting. I'm not sure how feasible it is, but it would be cool if it could be done. Basically, we want to look at pancreatic tumor markers to differentiate tumors which secrete hormones that are normally produced by the pancreas (ex. insulin) versus tumors which secrete hormones not usually produced by the pancreas (ex. growth hormone). Our hypothesis is that the former come from differentiated pancreatic cells, while the latter come from from pancreatic stem cells. The existence of pancreatic stem cells was only discovered quite recently, so it's a hot field.
This afternoon, I met with a researcher who I am considering working with for my research year. We discussed some possible ideas. I wasn't particularly gung ho about any of them, but he was open to me coming up with something else. So I really need to spend some time thinking about exactly what project I want to work on this spring and summer. Then I will need to start working on convincing someone to fund me for it. :-P
Wednesday, December 05, 2007
A Good ERB Day
This week's PBL case has been really interesting. I don't know who is writing the ERB PBL cases, but they're much better than the ones we had last block for NMS. These cases cover more ground, and we can't always predict from the getgo what is going to happen. We have even been getting into ethical issues like the pros and cons of genetic testing for the patient's children. It seems like an obviously helpful thing to do, but things aren't always that simple. What happens if there's not a clear treatment that would benefit the child, but now the child has this known genetic defect and can't get insurance as a young adult because the insurance company says he or she has a pre-existing condition? That doesn't even address the psychological distress that people can have due to knowing their genetic status. It makes more sense to do the testing if there is preventive care or screening that can be done, and also if the exact mutations are well-established. That didn't turn out to be the case for our patient though.
Today's seminars were on hypocalcemia and pituitary disorders. I was not initially excited about the hypocalcemia seminar, because it feels like we've beaten this stuff to death already. But it wound up being more interesting than I had expected. The speaker was the same guy who is in charge of our Friday POD seminars and who gave the semi-painful seminar on parathyroid differentiation proteins last week. He had assigned us to read a book chapter he wrote himself on pseudohypoparathyroidism, and it always makes me suspicious when profs do that. But I am glad I took the time to read it, because it goes into a lot more detail than Robbins (our path book) does.
Your body secretes parathyroid hormone (PTH) to keep your blood levels of calcium high enough. Calcium is very important for things like muscle contractions and intracellular signaling. It is so important to keep your blood calcium level high enough that your body will degrade your skeleton if necessary to accomplish this goal. That's where PTH comes in. If your blood levels of calcium get too low, you secrete PTH, and that causes your blood calcium to get higher by various mechanisms. People who have pseudohypoparathyroidism have low calcium levels, but it's not because they don't make enough PTH (which is the problem in true hypoparathyroidism). It's because their PTH receptors can't signal properly when PTH binds to them, which makes their blood calcium levels chronically low. Some patients are resistant to other hormones too since those receptors share some of the intracellular signaling machinery with the PTH receptor.
This afternoon, we had a communications session on patient education. One of my group members was absent and we didn't have a clinical correlation afterward, which means that we got out super early (2:30). So now I have the rest of this afternoon off. The three of us who were there were joking that one of us ought to volunteer to be absent from communications every time from now on. Also, it was snowing earlier, but now that has stopped too. Even though I am not a huge fan of snow, it really is beautiful while it's falling and when everything has just gotten covered with a fresh coat of it. Of course, it doesn't take too long for this whole city to get disgustingly dirty and icy slick, and that's when I start wishing I was going to med school in the Caribbean somewhere.
Today's seminars were on hypocalcemia and pituitary disorders. I was not initially excited about the hypocalcemia seminar, because it feels like we've beaten this stuff to death already. But it wound up being more interesting than I had expected. The speaker was the same guy who is in charge of our Friday POD seminars and who gave the semi-painful seminar on parathyroid differentiation proteins last week. He had assigned us to read a book chapter he wrote himself on pseudohypoparathyroidism, and it always makes me suspicious when profs do that. But I am glad I took the time to read it, because it goes into a lot more detail than Robbins (our path book) does.
Your body secretes parathyroid hormone (PTH) to keep your blood levels of calcium high enough. Calcium is very important for things like muscle contractions and intracellular signaling. It is so important to keep your blood calcium level high enough that your body will degrade your skeleton if necessary to accomplish this goal. That's where PTH comes in. If your blood levels of calcium get too low, you secrete PTH, and that causes your blood calcium to get higher by various mechanisms. People who have pseudohypoparathyroidism have low calcium levels, but it's not because they don't make enough PTH (which is the problem in true hypoparathyroidism). It's because their PTH receptors can't signal properly when PTH binds to them, which makes their blood calcium levels chronically low. Some patients are resistant to other hormones too since those receptors share some of the intracellular signaling machinery with the PTH receptor.
This afternoon, we had a communications session on patient education. One of my group members was absent and we didn't have a clinical correlation afterward, which means that we got out super early (2:30). So now I have the rest of this afternoon off. The three of us who were there were joking that one of us ought to volunteer to be absent from communications every time from now on. Also, it was snowing earlier, but now that has stopped too. Even though I am not a huge fan of snow, it really is beautiful while it's falling and when everything has just gotten covered with a fresh coat of it. Of course, it doesn't take too long for this whole city to get disgustingly dirty and icy slick, and that's when I start wishing I was going to med school in the Caribbean somewhere.
Tuesday, December 04, 2007
Too Many Tumors
Yesterday's seminars were both about tumors of the female reproductive tract. Today's were about tumors of the pituitary and adrenal glands. Our PBL case patient has tumors too. It's nice to know that people can get tumors of parts of the body that I didn't even know existed a year ago. On a happier note, most of these malignant endocrine tumors are fairly rare.
Today's FCM session was on motivational health promotion. My small group preceptor still wasn't back, but we had a sub this time, so I didn't luck out like last week. She started out by asking us how we were liking the class. I suggested that we just answer the questions we were supposed to answer and not discuss how we felt about the class. Luckily she didn't push the issue too much. As far as I'm concerned, it's irrelevant whether we like the class, because attending FCM is mandatory. We're all feeling tired, cranky, stressed, overworked, and ready for winter break. Take it for granted that every person in the room would rather be doing something else, and let's just get on with it. I don't want to even think about how lousy I feel right now, let alone have a whole gripe session about it.
The weather is bad today, so several of my patients didn't show up to clinic. I only wound up seeing two people. Of course, the ones who didn't show up were the 1:oo people, while naturally both of the 4:00 people came. We gave some flu shots and did some follow-ups, but all in all it wasn't a terribly exciting clinic day. I was sitting down while my preceptor talked to the last person, and it was tough for me to keep my eyes open. The room was kind of warm, and I was definitely doing that head jerk thing, so I decided that I'd better get up before I embarrassed myself.
Today's FCM session was on motivational health promotion. My small group preceptor still wasn't back, but we had a sub this time, so I didn't luck out like last week. She started out by asking us how we were liking the class. I suggested that we just answer the questions we were supposed to answer and not discuss how we felt about the class. Luckily she didn't push the issue too much. As far as I'm concerned, it's irrelevant whether we like the class, because attending FCM is mandatory. We're all feeling tired, cranky, stressed, overworked, and ready for winter break. Take it for granted that every person in the room would rather be doing something else, and let's just get on with it. I don't want to even think about how lousy I feel right now, let alone have a whole gripe session about it.
The weather is bad today, so several of my patients didn't show up to clinic. I only wound up seeing two people. Of course, the ones who didn't show up were the 1:oo people, while naturally both of the 4:00 people came. We gave some flu shots and did some follow-ups, but all in all it wasn't a terribly exciting clinic day. I was sitting down while my preceptor talked to the last person, and it was tough for me to keep my eyes open. The room was kind of warm, and I was definitely doing that head jerk thing, so I decided that I'd better get up before I embarrassed myself.
Saturday, December 01, 2007
Even My Blog Is for Sale!
I randomly stumbled upon an absolutely hysterical website today called BlogShares. Apparently they assign "market values" to blogs based on numbers of links and allow users to buy and sell shares in the blogs. My blog has mysteriously been listed on their site, and at the moment, is valued at B$1,000.00. This page explains how it works. At first, I didn't know whether to find this site to be disturbing or amusing, but the more I think about it, the funnier it gets. According to the website, I could register on Blogshares and stake my claim to my own blog as the owner, but it doesn't seem worth the trouble. I'll have to check back at some point though and see if anyone buys shares of my blog. :-)
Doc Opera was awesome. It's too bad the revisiting students don't get to come any more now that the show is in December instead of March. But for those of you who will be attending any of the Case programs next year, you should definitely at least go, and consider being in the show.
Doc Opera was awesome. It's too bad the revisiting students don't get to come any more now that the show is in December instead of March. But for those of you who will be attending any of the Case programs next year, you should definitely at least go, and consider being in the show.
Friday, November 30, 2007
More Bad Pregnancy Outcomes
Yesterday I had my MS class in the morning. We're getting close to the end now: only two more weeks to go. Not that I'm counting the days until I won't have to get up for a 7 AM class any more or anything. ;-)
Today we finished the PBL case about the HIV positive woman who wants to have a baby. The story has a partially positive ending. The baby isn't HIV-positive, but he does have a genetic abnormality. What really got people fired up though are the ethical issues, particularly one of this week's CAPPs that revolves around the issue of a pregnant patient who refuses care. That's a sticky issue, because you can't force a competent adult woman to receive needed medical care, but most people would also feel a desire to intervene to protect the fetus.
The seminars were about pre-eclampsia (a type of hypertension that pregnant women can get) and ectopic pregnancies (where the fetus doesn't implant in the uterus like it's supposed to). Not exactly the cheeriest subjects. Our POD/ARM talk was supposed to be about pregnancy related disorders, but instead it wound up being about a particular transcription factor (protein) that is expressed by cells that are "destined" to become parathyroid hormone cells. The researchers discovered that if they knocked this protein out in mice, some of the thymus cells became parathyroid type cells and started secreting parathyroid hormone. However, this does not happen in humans. Well, on the bright side, at least I'll know what to do in case I ever get a mouse that is deficient in this transcription factor coming into my office for help some day. And I also wrote my second essay for MS credit based on this talk, so it forced me to pay attention. Now I only have to do one more essay in January.
Tomorrow is Doc Opera already. I really enjoyed it last year, and I have been looking forward to this year's show.
Today we finished the PBL case about the HIV positive woman who wants to have a baby. The story has a partially positive ending. The baby isn't HIV-positive, but he does have a genetic abnormality. What really got people fired up though are the ethical issues, particularly one of this week's CAPPs that revolves around the issue of a pregnant patient who refuses care. That's a sticky issue, because you can't force a competent adult woman to receive needed medical care, but most people would also feel a desire to intervene to protect the fetus.
The seminars were about pre-eclampsia (a type of hypertension that pregnant women can get) and ectopic pregnancies (where the fetus doesn't implant in the uterus like it's supposed to). Not exactly the cheeriest subjects. Our POD/ARM talk was supposed to be about pregnancy related disorders, but instead it wound up being about a particular transcription factor (protein) that is expressed by cells that are "destined" to become parathyroid hormone cells. The researchers discovered that if they knocked this protein out in mice, some of the thymus cells became parathyroid type cells and started secreting parathyroid hormone. However, this does not happen in humans. Well, on the bright side, at least I'll know what to do in case I ever get a mouse that is deficient in this transcription factor coming into my office for help some day. And I also wrote my second essay for MS credit based on this talk, so it forced me to pay attention. Now I only have to do one more essay in January.
Tomorrow is Doc Opera already. I really enjoyed it last year, and I have been looking forward to this year's show.
Wednesday, November 28, 2007
Medical Genetics
I've been getting quite a lot of exposure to medical genetics lately. First, I did my learning objective for PBL on genetic counseling and ethics. As I mentioned yesterday, this week's case is about an HIV-positive woman who wants to have a baby. Obviously, there are many legal and ethical issues that would arise, from preventing transmission of HIV to the husband, to avoiding transmission to the infant, to genetic counseling of the woman for birth defects of the fetus. Today's seminar was on the use of drugs (both legal and illegal) during pregnancy, which isn't really related to genetics. But then this afternoon, I had genetics clinic.
Genetics clinic turned out to be pretty interesting. I expected most of the patients to be babies, but many aren't. They range in age from little kids all the way up to old people. We did see one baby who was developmentally delayed. But we also saw one woman in her thirties with an unknown genetic condition that caused her to be mentally retarded and have some other physical abnormalities. Probably the coolest patient was a teenager who had blue scleras due to type I osteogenesis imperfecta. (The whites of people's eyes who have this condition really do look noticeably bluish--see picture.) His family was there with him, and his dad and brother had blue scleras also, but they didn't have the same history of broken bones that the patient had. The medical geneticist took pictures of the patients after we examined them.
His family was there with him, and his dad and brother had blue scleras also, but they didn't have the same history of broken bones that the patient had. The medical geneticist took pictures of the patients after we examined them.
The one thing I felt kind of bad about is that I was so tired this afternoon that it was hard to stay focused. Medical genetics is very cool, like a detective hunt. We were looking up all kinds of info about genes on line in between patients. But the problem is that there is a lot of downtime, and I had a hard time staying awake. I just hope the preceptor didn't think I was bored, because I didn't feel that way at all. If I were going to go into internal medicine, medical genetics would definitely be one of the specialties I would consider.
Genetics clinic turned out to be pretty interesting. I expected most of the patients to be babies, but many aren't. They range in age from little kids all the way up to old people. We did see one baby who was developmentally delayed. But we also saw one woman in her thirties with an unknown genetic condition that caused her to be mentally retarded and have some other physical abnormalities. Probably the coolest patient was a teenager who had blue scleras due to type I osteogenesis imperfecta. (The whites of people's eyes who have this condition really do look noticeably bluish--see picture.)
 His family was there with him, and his dad and brother had blue scleras also, but they didn't have the same history of broken bones that the patient had. The medical geneticist took pictures of the patients after we examined them.
His family was there with him, and his dad and brother had blue scleras also, but they didn't have the same history of broken bones that the patient had. The medical geneticist took pictures of the patients after we examined them.The one thing I felt kind of bad about is that I was so tired this afternoon that it was hard to stay focused. Medical genetics is very cool, like a detective hunt. We were looking up all kinds of info about genes on line in between patients. But the problem is that there is a lot of downtime, and I had a hard time staying awake. I just hope the preceptor didn't think I was bored, because I didn't feel that way at all. If I were going to go into internal medicine, medical genetics would definitely be one of the specialties I would consider.
Tuesday, November 27, 2007
Reproductive Biology
This week we started reproductive medicine. Our PBL case is about another couple that is trying to get pregnant--this time, the woman is HIV-positive and the man is HIV-negative. The woman also has genital warts. These viral infections certainly add to the complexity of the case. The seminars are about all of the things that can go wrong with pregnancy. All I can say is that no sane woman should go to medical school until AFTER she has her kids. There is definitely such a thing as having too much information! Yesterday we talked about some of the infections that pregnant women can get, and today we learned about fetal genetic defects and placental problems. I have a much better appreciation now about why pregnancy is so dangerous for women. Throw in all of the genetic defects that the fetus can have, and it's amazing any pregnancy ever comes out right at all.
Our FCM seminar today was about alternative and complementary medicine. My group's preceptor didn't show up, so after twenty minutes I went to the library to read. That was an extra hour of reading time that I hadn't expected, but it was greatly appreciated. I'm actually going to be completely prepared for tomorrow's seminar.
We were really busy in clinic today. My preceptor and I used to only see six people on my clinic days, but now we're seeing seven patients each day due to a new departmental policy. You wouldn't think that adding one more patient to the schedule would be that big of a deal, but they are adding the last patient in the 4:00 time slot. So now the two of us really have to push to get everything done at the end. I saw five patients instead of my usual four. There was one diabetic, one with migraine headaches, one with a cold, one with moles that "looked funny," and one who just needed a checkup. It was a busy day, but I suppose I should be grateful that there wasn't anyone who was trying to get pregnant!
Our FCM seminar today was about alternative and complementary medicine. My group's preceptor didn't show up, so after twenty minutes I went to the library to read. That was an extra hour of reading time that I hadn't expected, but it was greatly appreciated. I'm actually going to be completely prepared for tomorrow's seminar.
We were really busy in clinic today. My preceptor and I used to only see six people on my clinic days, but now we're seeing seven patients each day due to a new departmental policy. You wouldn't think that adding one more patient to the schedule would be that big of a deal, but they are adding the last patient in the 4:00 time slot. So now the two of us really have to push to get everything done at the end. I saw five patients instead of my usual four. There was one diabetic, one with migraine headaches, one with a cold, one with moles that "looked funny," and one who just needed a checkup. It was a busy day, but I suppose I should be grateful that there wasn't anyone who was trying to get pregnant!
Wednesday, November 21, 2007
Happy Thanksgiving!
I found out today that the UP students had this whole week off, the lucky dogs. I can't complain though, because at least I got out of having clinic this afternoon. I was supposed to have breast clinic, but I withdrew because I would rather do genetics clinic next week. I've already done enough breast exams in clinic to last me a lifetime.
Both of our seminars today were yet again depressing, on cervical and uterine cancers. At least the PBL case had a happy ending. We were pretty rushed though since we had eight learning objectives plus three parts of the case to go through, and we had to fill out the weekly eval today too. I was unlucky enough to be the group leader this week, and although it was rushed, somehow we managed to get everything done more or less on time.
Anyway, I have the rest of this week off and I plan to enjoy it. I'm going for dinner with friends tonight and having Thanksgiving at a friend's house tomorrow. We have SAQs to do this weekend but no CAPPs. It really WILL almost be like a vacation. :-P
Both of our seminars today were yet again depressing, on cervical and uterine cancers. At least the PBL case had a happy ending. We were pretty rushed though since we had eight learning objectives plus three parts of the case to go through, and we had to fill out the weekly eval today too. I was unlucky enough to be the group leader this week, and although it was rushed, somehow we managed to get everything done more or less on time.
Anyway, I have the rest of this week off and I plan to enjoy it. I'm going for dinner with friends tonight and having Thanksgiving at a friend's house tomorrow. We have SAQs to do this weekend but no CAPPs. It really WILL almost be like a vacation. :-P
Tuesday, November 20, 2007
Spiritual Madness
Today was one of those crazy days where I think back on it later and kind of just shake my head. We had not one, not two, but THREE seminars this morning about prostate and testicular pathology. They were one after another, each with its own reading. All of them were great seminars, but three in a row was just a little over the top.
Then there was FCM. They had this guy from pastoral care come to give us a seminar. He was supposed to be talking about spirituality and how it affects decision-making in medicine. Instead, he wound up getting into a fight with about half the students in my class and half the preceptors too, because he was saying things like that ministers are the only people with proper training to help patients spiritually. That really got the doctors' dander up. He was also asking ridiculous questions like how we thought the case patient felt when she was having sex at the age of 11. Ok, first of all, this case patient is a composite, not a real person. Second of all, it's not like she was there and we could ask her! How the heck would we know what an imaginary person felt while having sex twenty years ago? The whole exchange was very hostile, and the FCM faculty wound up emailing the entire class this afternoon to apologize for the speaker's behavior. We didn't learn much, but at least for once I can say that an FCM session was exciting!
I had clinic in the afternoon. When I got there, it turned out that my preceptor was on vacation all this week and no one had told me. The nurses said I could go home, but I didn't want to have to make up the clinic. So I wound up working with one of the residents and his preceptor instead. He had a patient who needed a neuro exam, and he let me do it. At long last, I pretty much have the cranial nerve exam down, and no one has to prompt me because I forgot to examine CN 11 or something.
There is a pharmacist in our clinic who meets with patients, and I went into a room with her resident on one patient also. That was really interesting because I had no idea what the pharmacists did in the clinic. It turns out that they counsel patients with tough cases who take lots of meds. This particular patient was a diabetic who was completely noncompliant and was also hypertensive, obese, and dyslipidemic. The most interesting part to me was how different the focus was. The pharmacists really don't get much into the disease symptoms or mechanisms at all. After the resident presented to the senior, they were debating for 15 minutes about which type of insulin was best for this patient, and so I got a review of all the different long and short-acting insulins. When they were done, the pharmacist asked me what I thought we should do. I said, "Tell the patient to drink diet soda instead of regular soda." All the insulin in the world is not going to help a patient who drinks a six pack of sugar water every day!
Then there was FCM. They had this guy from pastoral care come to give us a seminar. He was supposed to be talking about spirituality and how it affects decision-making in medicine. Instead, he wound up getting into a fight with about half the students in my class and half the preceptors too, because he was saying things like that ministers are the only people with proper training to help patients spiritually. That really got the doctors' dander up. He was also asking ridiculous questions like how we thought the case patient felt when she was having sex at the age of 11. Ok, first of all, this case patient is a composite, not a real person. Second of all, it's not like she was there and we could ask her! How the heck would we know what an imaginary person felt while having sex twenty years ago? The whole exchange was very hostile, and the FCM faculty wound up emailing the entire class this afternoon to apologize for the speaker's behavior. We didn't learn much, but at least for once I can say that an FCM session was exciting!
I had clinic in the afternoon. When I got there, it turned out that my preceptor was on vacation all this week and no one had told me. The nurses said I could go home, but I didn't want to have to make up the clinic. So I wound up working with one of the residents and his preceptor instead. He had a patient who needed a neuro exam, and he let me do it. At long last, I pretty much have the cranial nerve exam down, and no one has to prompt me because I forgot to examine CN 11 or something.
There is a pharmacist in our clinic who meets with patients, and I went into a room with her resident on one patient also. That was really interesting because I had no idea what the pharmacists did in the clinic. It turns out that they counsel patients with tough cases who take lots of meds. This particular patient was a diabetic who was completely noncompliant and was also hypertensive, obese, and dyslipidemic. The most interesting part to me was how different the focus was. The pharmacists really don't get much into the disease symptoms or mechanisms at all. After the resident presented to the senior, they were debating for 15 minutes about which type of insulin was best for this patient, and so I got a review of all the different long and short-acting insulins. When they were done, the pharmacist asked me what I thought we should do. I said, "Tell the patient to drink diet soda instead of regular soda." All the insulin in the world is not going to help a patient who drinks a six pack of sugar water every day!
Monday, November 19, 2007
The Problems of Women and Men
So far this has been a very depressing week as far as classes go. Our PBL case patient has genital warts and cervical cancer. The two seminars today, although interesting and well-done, were about breast cancer. This is going to go on for the rest of the week--tomorrow, we're covering male genitourinary problems, and Wednesday we're back to women. One interesting thing I noticed is that our pathology book has tons more coverage of women's health problems than men's. There are two separate chapters on women's health, one just on breast diseases and another huge one about diseases of the female reproductive tract. The sole men's health chapter is much shorter. I wonder if this is because there are that many more diseases of the female reproductive tract, or if we just know more about women's diseases?
Speaking of genitourinary tracts, this evening I did my GU exams at the Cleveland Free Clinic. It was quite an experience. Two of my classmates and I got there at 4:45, and we first got a pep talk of sorts by the woman who coordinates the medical student practice exams. She spent about half an hour telling us that we had to be professional, and giving us all kinds of ideas of how NOT to be professional that I would never have been clever enough to have come up with on my own if she hadn't described them in excruciating detail. Like, apparently in the past some med students have said they were going to the bathroom, but then bailed instead without telling anyone. She warned us not to sneak out of the clinic, or she'd have to report us to the school. I had to laugh, because as much as I was not looking forward to performing a digital rectal exam, I haven't come this far and worked this hard to let something like this stop me from getting my MD. So none of us bailed, and we managed to mostly stay awake during an incredibly boring video about Pap smears that, judging from the clothing the actors wore and the equipment being used, must have been made in the late 70s or early 80s.
After an hour of these torments, we were finally ready to do the female exam. Since there were three of us students, we were divided into one pair and one single person. I was the single person, and I had a sort of coach in the room to help me along with the patient herself. My standardized patient and the coach were super helpful, and once they started giving me instructions I got over the weirdness of the situation pretty quickly. First, we went through the breast exam, which I had done several times in longitudinal clinic already. No biggie. Then it was time for the pelvic exam. (We inserted the speculum, but didn't do the actual Pap smear.) I inserted the speculum and was able to visualize the os (opening) of her cervix on the first try. Then I tried to palpate her ovaries (I couldn't really feel them) and did the rectal exam. It wasn't too bad because I was so focused on what I was doing that I didn't even think about the grossness factor.
All that was left to do was the male exam. Since I was done first, I got to spend another 20 minutes one-on-one with the coordinator lady and hear about more blunders committed by previous medical students over the years. When the male standardized patients arrived, one of my classmates and I were paired together this time. That standardized patient was really awesome also. He started by explaining the exam, and then I went first. The male exam was a lot more uncomfortable for me than the female exam. The man was standing in front of me, and I was inspecting his penis and testes while seated, which felt pretty awkward. The weirdest part was when I was examining for an inguinal hernia. He didn't have a hernia, so I had to palpate pretty deeply into his inguinal canal to reach the inguinal ring. When he coughed I could actually feel his intestines move. After my classmate repeated the exam, we moved on to examining the prostate, which entailed yet another digital rectal exam. I was able to palpate the prostate, but it was hard to reach the far edges. Prostates are larger than I had realized.
We were finished at 9:00, and I was definitely glad to be done. Doing the GU exams wasn't as awful as some people make them out to be--you're so busy concentrating on the exam that you don't really have time to sit there and think about how gross it is. But at the same time, I am absolutely certain that I have zero desire to go into either gynecology or urology. Even though doing the GU exams wasn't all that big of a deal, I am definitely not looking to make a career out of it.
Speaking of genitourinary tracts, this evening I did my GU exams at the Cleveland Free Clinic. It was quite an experience. Two of my classmates and I got there at 4:45, and we first got a pep talk of sorts by the woman who coordinates the medical student practice exams. She spent about half an hour telling us that we had to be professional, and giving us all kinds of ideas of how NOT to be professional that I would never have been clever enough to have come up with on my own if she hadn't described them in excruciating detail. Like, apparently in the past some med students have said they were going to the bathroom, but then bailed instead without telling anyone. She warned us not to sneak out of the clinic, or she'd have to report us to the school. I had to laugh, because as much as I was not looking forward to performing a digital rectal exam, I haven't come this far and worked this hard to let something like this stop me from getting my MD. So none of us bailed, and we managed to mostly stay awake during an incredibly boring video about Pap smears that, judging from the clothing the actors wore and the equipment being used, must have been made in the late 70s or early 80s.
After an hour of these torments, we were finally ready to do the female exam. Since there were three of us students, we were divided into one pair and one single person. I was the single person, and I had a sort of coach in the room to help me along with the patient herself. My standardized patient and the coach were super helpful, and once they started giving me instructions I got over the weirdness of the situation pretty quickly. First, we went through the breast exam, which I had done several times in longitudinal clinic already. No biggie. Then it was time for the pelvic exam. (We inserted the speculum, but didn't do the actual Pap smear.) I inserted the speculum and was able to visualize the os (opening) of her cervix on the first try. Then I tried to palpate her ovaries (I couldn't really feel them) and did the rectal exam. It wasn't too bad because I was so focused on what I was doing that I didn't even think about the grossness factor.
All that was left to do was the male exam. Since I was done first, I got to spend another 20 minutes one-on-one with the coordinator lady and hear about more blunders committed by previous medical students over the years. When the male standardized patients arrived, one of my classmates and I were paired together this time. That standardized patient was really awesome also. He started by explaining the exam, and then I went first. The male exam was a lot more uncomfortable for me than the female exam. The man was standing in front of me, and I was inspecting his penis and testes while seated, which felt pretty awkward. The weirdest part was when I was examining for an inguinal hernia. He didn't have a hernia, so I had to palpate pretty deeply into his inguinal canal to reach the inguinal ring. When he coughed I could actually feel his intestines move. After my classmate repeated the exam, we moved on to examining the prostate, which entailed yet another digital rectal exam. I was able to palpate the prostate, but it was hard to reach the far edges. Prostates are larger than I had realized.
We were finished at 9:00, and I was definitely glad to be done. Doing the GU exams wasn't as awful as some people make them out to be--you're so busy concentrating on the exam that you don't really have time to sit there and think about how gross it is. But at the same time, I am absolutely certain that I have zero desire to go into either gynecology or urology. Even though doing the GU exams wasn't all that big of a deal, I am definitely not looking to make a career out of it.
Friday, November 16, 2007
Conferences, Incontinence, and In Vitro Fertilization
The conference I went to yesterday was really good, but I'm glad it's the last one that I'll be attending for a while. It's amazing how much these conferences totally screwed up my schedule. I also missed my MS class (which I have to confess that I'm not especially sorry about) and a Dean's Dinner by Steve Nissen (which I am definitely sorry about). That was the first Dean's Dinner that I've missed since I started med school, and I would have loved to have gone. I've seen him talk once before about his work on intravascular ultrasound, and he was supposed to discuss that again last night. But apparently he wound up discussing the whole Avandia brouhaha due to his meta-analysis that was published earlier this year.
Our PBL case had a very happy ending, and our only seminar today was anatomy. This was a review of the genitourinary systems of the male and female. The talk at the beginning was about different kinds of urinary incontinence. One type, called stress incontinence, can happen due to an anatomic problem when pressure increases in the abdomen (ex. from laughing or coughing). The other type is urge incontinence, which is due to a neurological type of problem. The difference is important because urge incontinence can be treated medically, while stress incontinence tends not to respond to medication and has to be fixed surgically.
I met with my PA also and we discussed my portfolio essay and my plans for next year. Right now I am tentatively planning to do Core I (medicine and surgery) starting in July, then a block of research and electives starting in November, and then Core II (neuro/ob/gyn/psych/peds) in March. I would probably then do my Advanced Cores in July of my fourth year and start my research year afterward in November. This will give me time to write a proposal and get it approved by the CCF IRB.
Our POD speaker today (sorry, our ARM speaker today) is doing research in infertility and in vitro fertilization. He was a really engaging speaker who told us a bunch of interesting anecdotes about the early days of in vitro fertilization. For example, he was involved with the first in vitro fertilization that was done in the state of Ohio, which was in 1983, and he was the first person in the world to implant an in vitro-fertilized embryo into a surrogate mother. Currently he has a project that raises money to help pay for gamete storage and in vitro fertilization for lower-income patients who could not otherwise afford it. The program particularly targets young female cancer patients who are undergoing radiation that could render them infertile and incapable of having children at a later date.
The talk was certainly enjoyable and the research was very interesting. But I can't quite push this nagging thought out of my mind that as frustrating as infertility must be to people who really want a child, it's maybe not the most pressing problem in all of medicine. Why should in vitro fertilization deserve so much of our limited supplies of funding and brainpower? No woman is going to die if she can't become pregnant, and couples who cannot have their own biological children can always adopt a child. I'm not saying that this kind of research shouldn't be done or that the technology for in vitro fertilization shouldn't be used. It's just that there are plenty of life-threatening problems that could possibly be ameliorated by setting up foundations to subsidize health care costs for lower-income people whose jobs don't provide them with health insurance. For example, why isn't there a foundation to subsidize yearly Pap smears for low-income women so that they don't die of cervical cancer that could have been treatable if it had been caught earlier?
Our PBL case had a very happy ending, and our only seminar today was anatomy. This was a review of the genitourinary systems of the male and female. The talk at the beginning was about different kinds of urinary incontinence. One type, called stress incontinence, can happen due to an anatomic problem when pressure increases in the abdomen (ex. from laughing or coughing). The other type is urge incontinence, which is due to a neurological type of problem. The difference is important because urge incontinence can be treated medically, while stress incontinence tends not to respond to medication and has to be fixed surgically.
I met with my PA also and we discussed my portfolio essay and my plans for next year. Right now I am tentatively planning to do Core I (medicine and surgery) starting in July, then a block of research and electives starting in November, and then Core II (neuro/ob/gyn/psych/peds) in March. I would probably then do my Advanced Cores in July of my fourth year and start my research year afterward in November. This will give me time to write a proposal and get it approved by the CCF IRB.
Our POD speaker today (sorry, our ARM speaker today) is doing research in infertility and in vitro fertilization. He was a really engaging speaker who told us a bunch of interesting anecdotes about the early days of in vitro fertilization. For example, he was involved with the first in vitro fertilization that was done in the state of Ohio, which was in 1983, and he was the first person in the world to implant an in vitro-fertilized embryo into a surrogate mother. Currently he has a project that raises money to help pay for gamete storage and in vitro fertilization for lower-income patients who could not otherwise afford it. The program particularly targets young female cancer patients who are undergoing radiation that could render them infertile and incapable of having children at a later date.
The talk was certainly enjoyable and the research was very interesting. But I can't quite push this nagging thought out of my mind that as frustrating as infertility must be to people who really want a child, it's maybe not the most pressing problem in all of medicine. Why should in vitro fertilization deserve so much of our limited supplies of funding and brainpower? No woman is going to die if she can't become pregnant, and couples who cannot have their own biological children can always adopt a child. I'm not saying that this kind of research shouldn't be done or that the technology for in vitro fertilization shouldn't be used. It's just that there are plenty of life-threatening problems that could possibly be ameliorated by setting up foundations to subsidize health care costs for lower-income people whose jobs don't provide them with health insurance. For example, why isn't there a foundation to subsidize yearly Pap smears for low-income women so that they don't die of cervical cancer that could have been treatable if it had been caught earlier?
Wednesday, November 14, 2007
PBL, Pharm, Peds Clinic, and Portfolio
Today's portion of the CCLCM curriculum is obviously sponsored by the letter P.
Our PBL case took a little twist that seems kind of farfetched, but at least it kept things interesting. I wasn't able to find any good pictures about my learning objective topic, so I had to do a "chalk talk" for my presentation. The only reason I don't like doing that is because then there's nothing for people to look at later on the portal, but it couldn't be helped. After PBL, we had a seminar about contraceptives. I like the pharmacist who led the seminar, but this seminar didn't seem to go very smoothly. She has led other seminars for us before, and I don't remember them being this disjointed. We had a lot of time in between discussing questions where we were supposed to be looking things up in small groups, but I don't feel like I got as much out of it as usual, and people weren't participating much today. Maybe it's a general feeling of being tired and ready for Thanksgiving, and plus our first portfolios are due tomorrow. I already finished mine and submitted it. I had to get it done early because I'm going to a conference tomorrow.
Peds clinic this afternoon was great again. I was working with the same adolescent medicine specialist that I worked with last time, and we saw a bunch of really interesting cases. This time there were a couple of little kids thrown in there too, and I even enjoyed examining them since they weren't screaming. The one kid who did scream was an older kid who I swear had a temper tantrum right there in the doctor's office, but luckily I didn't have to examine that one. There's something particularly irritating to me about really little kids screaming--I think it's just that their screams are so shrill. Even though I really like adolescent medicine, I'm not sure I'd realistically survive a three year peds residency.
Our PBL case took a little twist that seems kind of farfetched, but at least it kept things interesting. I wasn't able to find any good pictures about my learning objective topic, so I had to do a "chalk talk" for my presentation. The only reason I don't like doing that is because then there's nothing for people to look at later on the portal, but it couldn't be helped. After PBL, we had a seminar about contraceptives. I like the pharmacist who led the seminar, but this seminar didn't seem to go very smoothly. She has led other seminars for us before, and I don't remember them being this disjointed. We had a lot of time in between discussing questions where we were supposed to be looking things up in small groups, but I don't feel like I got as much out of it as usual, and people weren't participating much today. Maybe it's a general feeling of being tired and ready for Thanksgiving, and plus our first portfolios are due tomorrow. I already finished mine and submitted it. I had to get it done early because I'm going to a conference tomorrow.
Peds clinic this afternoon was great again. I was working with the same adolescent medicine specialist that I worked with last time, and we saw a bunch of really interesting cases. This time there were a couple of little kids thrown in there too, and I even enjoyed examining them since they weren't screaming. The one kid who did scream was an older kid who I swear had a temper tantrum right there in the doctor's office, but luckily I didn't have to examine that one. There's something particularly irritating to me about really little kids screaming--I think it's just that their screams are so shrill. Even though I really like adolescent medicine, I'm not sure I'd realistically survive a three year peds residency.
Tuesday, November 13, 2007
Endo/Repro Block, Round II
Yesterday was our first day of Endocrinology and Reproductive Biology (ERB). Evidently the ERB faculty have decided to follow the NMS pattern and give us two seminars per day. That would be fine--it would be great, actually--if they didn't also double the reading we're supposed to do! It's absolutely impossible to get it all done and still have time to eat, breathe, and sleep. I'm at about half done, half not so far this week.
Yesterday's seminars were on uterus pathology and pain during menstruation, and today's were on male hormones and menstrual disorders. So far they've all been well done on the whole. Our PBL case this week is good too. It's about an infertile couple, so there are a lot of potential problems in our differential. I really like my new PBL tutor. We're his first group, but he's a lot more involved than my tutor last block was, and yesterday's session went noticeably smoother versus last block. Today's FCM session was about improving performance measurements to increase the quality of health care systems, which has to be one of the least interesting topics I can possibly imagine. I know it's an important issue, and I understand why I should know something about it, but I can't say that I'm particularly fired up about which methods we can use to assess hospital performance.
My observed history and physical (H & P) was today, and it went really well. I had an hour and a half to get my patient's history and examine her while my preceptor sat in the corner and kept track of what I was doing. (This was a real patient, not a standardized patient.) The patient was really funny. When I went through the review of systems, she pretty much had every problem I asked about. She also was one of those patients who likes to go off on tangents, so I had to use a lot of closed-ended questions to keep her on track so I wouldn't run over time. There were a few things that I forgot to ask about (family history, illegal drug use) and do (listen for murmurs in the carotid arteries of the neck). But overall my preceptor was happy with how I did and gave me a really good eval. And this time, I did remember to examine both the heart and the liver from the patient's right side. :-) After the H & P, I had an hour to write it up and then 15 minutes to present it to my preceptor. I had to make a few corrections before submitting my final copy, and I'm done.
My take-home exam from the summer epidemiology class is due on Thursday, but I'm pretty much done with it. There was one question that I am pretty sure I got wrong, but I don't know how to fix it, and I am not allowed to ask anyone for help. Hopefully I'm at least on the right track, but at this point I am pretty much out of time and just need to turn it in.
Yesterday's seminars were on uterus pathology and pain during menstruation, and today's were on male hormones and menstrual disorders. So far they've all been well done on the whole. Our PBL case this week is good too. It's about an infertile couple, so there are a lot of potential problems in our differential. I really like my new PBL tutor. We're his first group, but he's a lot more involved than my tutor last block was, and yesterday's session went noticeably smoother versus last block. Today's FCM session was about improving performance measurements to increase the quality of health care systems, which has to be one of the least interesting topics I can possibly imagine. I know it's an important issue, and I understand why I should know something about it, but I can't say that I'm particularly fired up about which methods we can use to assess hospital performance.
My observed history and physical (H & P) was today, and it went really well. I had an hour and a half to get my patient's history and examine her while my preceptor sat in the corner and kept track of what I was doing. (This was a real patient, not a standardized patient.) The patient was really funny. When I went through the review of systems, she pretty much had every problem I asked about. She also was one of those patients who likes to go off on tangents, so I had to use a lot of closed-ended questions to keep her on track so I wouldn't run over time. There were a few things that I forgot to ask about (family history, illegal drug use) and do (listen for murmurs in the carotid arteries of the neck). But overall my preceptor was happy with how I did and gave me a really good eval. And this time, I did remember to examine both the heart and the liver from the patient's right side. :-) After the H & P, I had an hour to write it up and then 15 minutes to present it to my preceptor. I had to make a few corrections before submitting my final copy, and I'm done.
My take-home exam from the summer epidemiology class is due on Thursday, but I'm pretty much done with it. There was one question that I am pretty sure I got wrong, but I don't know how to fix it, and I am not allowed to ask anyone for help. Hopefully I'm at least on the right track, but at this point I am pretty much out of time and just need to turn it in.
Friday, November 09, 2007
Last Day of Neuro Block!
So amazingly, I have survived this entire NMS block, and sometimes I actually even liked it. All three of our PBL "caselets" for this week ended happily, including the noncompliant patient, who suddenly saw the light and became compliant. Obviously, this PBL case is not totally true to life! The seminar was about vision. Although the speaker was good, I had a hard time focusing. I just wasn't very mentally with it today, and it didn't help that I hadn't been able to get any of today's reading assignment done ahead of time.
Our POD speaker was FANTASTIC. His talk was supposed to be about pain, but instead he was discussing the relationship between depression and cardiovascular disease. Apparently in both cases, there are cytokines (inflammatory immune system proteins) that get upregulated. It isn't known if that is a cause or an effect, but in either case, people who are depressed tend to have more cardiovascular disease, and people who have cardiovascular disease have worse prognoses if they are depressed. I was thinking about this idea of inflammatory cytokines being related to cardiovascular disease and depression, and it hit me that if this hypothesis is true, then people with autoimmune disorders like rheumatoid arthritis ought to have a greater risk of depression and cardiovascular disease. I looked it up, and sure enough, they do. I wound up designing an experiment and writing an essay around this idea. I am required to write three of these essays (just 1-2 pages each) in order to get MS credit for the POD course, so now I only have two left to do.
Our POD speaker was FANTASTIC. His talk was supposed to be about pain, but instead he was discussing the relationship between depression and cardiovascular disease. Apparently in both cases, there are cytokines (inflammatory immune system proteins) that get upregulated. It isn't known if that is a cause or an effect, but in either case, people who are depressed tend to have more cardiovascular disease, and people who have cardiovascular disease have worse prognoses if they are depressed. I was thinking about this idea of inflammatory cytokines being related to cardiovascular disease and depression, and it hit me that if this hypothesis is true, then people with autoimmune disorders like rheumatoid arthritis ought to have a greater risk of depression and cardiovascular disease. I looked it up, and sure enough, they do. I wound up designing an experiment and writing an essay around this idea. I am required to write three of these essays (just 1-2 pages each) in order to get MS credit for the POD course, so now I only have two left to do.
Thursday, November 08, 2007
Visiting an Abortion Clinic
Today was quite an interesting day. I had my MS class this morning, and it was actually enjoyable. The same statistician that I really liked last summer gave the first half of the class, and one of the statisticians I had worked with over the summer for my research gave the other half.
Last week, one of my classmates had invited all of the CCLCM students to visit Preterm, which is an abortion clinic about ten minutes away from CCF in Shaker Square. There is a student group for choice at Case, and a bunch of Case students went today, along with about half a dozen of us from CCLCM. Visiting an abortion clinic was both a disturbing and informative experience, and it's probably something that every medical student nationwide ought to do.
The clinic staff began by giving us an orientation to the clinic and what services are provided there. (They provide counseling services and birth control as well as abortions.) We were also given statistics about abortions, abortion access, and political efforts to keep abortion legal versus outlaw it. One thing I hadn't realized is that Ohio has a pretty extreme, staunchly anti-choice state legislature. One representative apparently introduced a bill that would outlaw all abortions, even if it was necessary to save the life of the woman. They also passed around a pro-choice petition for people to sign. I am not registered to vote in Ohio, so it wasn't an issue for me to decide if I even wanted to support pro-choice legislation, but I'm not sure I would have signed regardless. That is mainly because I felt the orientation was a bit overly proselytistic and defensive. But I suppose it's understandable that it would be, considering that the clinic employees have rude protesters outside their place of work shouting nasty things at them and their clients every day.
The more interesting part was when the staff demonstrated how the abortions were done. I didn't know very much about abortion procedures before visiting the clinic, and the surgery procedure in particular was nothing like what I expected. Most women get abortions during their first trimester using vacuum aspiration. The abortion is performed by first dilating their cervix, and then inserting the vacuum cannula and suctioning the embryo out of there. It only takes a few minutes to do the suctioning from start to finish, and no further surgery is required. They had models of a woman's cervix and manual vacuum pumps that were basically like giant syringes so that we could see what it was like to perform the procedure ourselves. It was surprisingly easy to do once I got the hang of using the vacuum pump.
Alternatively, the patient can be given a medical abortion using drugs that interfere with progesterone activity and prostaglandins, which stimulate uterine contraction. (Progesterone is the hormone that maintains the uterine lining during pregnancy.) She takes one pill at the clinic and then a second one at home the following day. This method of abortion actually has a higher rate of complication versus the first method.
If the woman is past her first trimester, other methods like dilation and evacuation (D & E) have to be used. These are the infamous "partial birth" abortions, where the woman's cervix is dilated, and then the fetus is partially delivered, disassembled and pulled out of the uterus piece by piece. The physician described the procedure to us, and it was pretty graphic and gruesome. He explained that although Congress tried to outlaw D & E a few years ago, it is still performed in this country. The main difference is that they apparently used to do it on a living fetus, and now they are required to kill the fetus first before removing it from the woman's uterus.
I can't agree with what I view as Preterm's completely amoral stance about abortion. As a person who is devoting my life to "doing no harm," I do consider abortion to be a "necessary evil," and I do not agree that abortion is just another form of birth control. Unplanned pregnancies are tragic, and so are the abortions themselves. If that makes me "judgmental," then I suppose I am guilty as charged.
Last week, one of my classmates had invited all of the CCLCM students to visit Preterm, which is an abortion clinic about ten minutes away from CCF in Shaker Square. There is a student group for choice at Case, and a bunch of Case students went today, along with about half a dozen of us from CCLCM. Visiting an abortion clinic was both a disturbing and informative experience, and it's probably something that every medical student nationwide ought to do.
The clinic staff began by giving us an orientation to the clinic and what services are provided there. (They provide counseling services and birth control as well as abortions.) We were also given statistics about abortions, abortion access, and political efforts to keep abortion legal versus outlaw it. One thing I hadn't realized is that Ohio has a pretty extreme, staunchly anti-choice state legislature. One representative apparently introduced a bill that would outlaw all abortions, even if it was necessary to save the life of the woman. They also passed around a pro-choice petition for people to sign. I am not registered to vote in Ohio, so it wasn't an issue for me to decide if I even wanted to support pro-choice legislation, but I'm not sure I would have signed regardless. That is mainly because I felt the orientation was a bit overly proselytistic and defensive. But I suppose it's understandable that it would be, considering that the clinic employees have rude protesters outside their place of work shouting nasty things at them and their clients every day.
The more interesting part was when the staff demonstrated how the abortions were done. I didn't know very much about abortion procedures before visiting the clinic, and the surgery procedure in particular was nothing like what I expected. Most women get abortions during their first trimester using vacuum aspiration. The abortion is performed by first dilating their cervix, and then inserting the vacuum cannula and suctioning the embryo out of there. It only takes a few minutes to do the suctioning from start to finish, and no further surgery is required. They had models of a woman's cervix and manual vacuum pumps that were basically like giant syringes so that we could see what it was like to perform the procedure ourselves. It was surprisingly easy to do once I got the hang of using the vacuum pump.
Alternatively, the patient can be given a medical abortion using drugs that interfere with progesterone activity and prostaglandins, which stimulate uterine contraction. (Progesterone is the hormone that maintains the uterine lining during pregnancy.) She takes one pill at the clinic and then a second one at home the following day. This method of abortion actually has a higher rate of complication versus the first method.
If the woman is past her first trimester, other methods like dilation and evacuation (D & E) have to be used. These are the infamous "partial birth" abortions, where the woman's cervix is dilated, and then the fetus is partially delivered, disassembled and pulled out of the uterus piece by piece. The physician described the procedure to us, and it was pretty graphic and gruesome. He explained that although Congress tried to outlaw D & E a few years ago, it is still performed in this country. The main difference is that they apparently used to do it on a living fetus, and now they are required to kill the fetus first before removing it from the woman's uterus.
I can't agree with what I view as Preterm's completely amoral stance about abortion. As a person who is devoting my life to "doing no harm," I do consider abortion to be a "necessary evil," and I do not agree that abortion is just another form of birth control. Unplanned pregnancies are tragic, and so are the abortions themselves. If that makes me "judgmental," then I suppose I am guilty as charged.
Wednesday, November 07, 2007
PBL, Hearing, Vestibular, and Clinical Correlations
Today's PBL session was kind of nuts. We had a few other mini cases besides the one we started on Monday, and it was just really disjointed. "After seeing Patient A and prescribing her medication Y, Dr. X goes into the next room to see patient B. Patient B's symptoms are...." So it wound up being a list of symptoms that we used to figure out what kind of headaches the patients were having. We found one of the patient descriptions almost word-for-word on the internet. I don't know if that says more about the case writer's lack of creativity or the medical students' mad googling skills.
I didn't get a chance to do the reading for either seminar today, but it was ok because I was able to skim through the chapters during the seminars. The first seminar was about the vestibular system, and the seminar leader, although a nice guy and clearly trying to do his best, was way overambitious. He had 69 slides for a 50-minute seminar! Unsurprisingly, he had to deliver his talk at breakneck speed, and we ran way over. The second seminar was about hearing. It was given by two audiologists. I hadn't realized that any audiologists worked at CCF, but there are at least two. Audiologists treat patients with hearing or vestibular problems, but they aren't physicians. They have their own degree called a doctorate of audiology. These two audiologists were both really nice too, but their seminar had the opposite problem--it was kind of repetitive and not the most interesting.
In the afternoon, I had two clinical correlations. The first one was for doing neurological exams on patients with neuro disorders, and it was really great. We saw patients with Parkinson's disease (PD) and multiple sclerosis. One of the PD patients has a deep brain stimulator (DBS) implanted, and he turned it off for us so that we could see how bad his tremors were without it. DBS is incredibly cool technology and its use in PD is becoming more common. In a nutshell, the patient gets a sort of pacemaker implanted into an area of their brain called the globus pallidus. The neurons there are part of a movement pathway from another area called the substantia nigra, and neurons from the substantia nigra get destroyed in PD. The pathways are pretty complex, but the end result is a lack of volitional movement, and that's what DBS can help overcome. (If you're interested in DBS, you can read more about it here.)
The second clinical correlation wasn't very good, but apparently some of the other groups had a better experience. My group wound up waiting for half an hour at the desk in the neuro ICU. The secretary paged the doctor for us, and he said he would come get us, but no one ever came. So finally, we started wandering around the neuro ICU until we ran into another doc who took us in to see one of the comatose patients and went through the general procedure of how they examine these patients. We didn't get to actually examine the patient though, and I didn't really get much out of it. It was especially hard to concentrate on what the doctor was saying because the TV was blaring overhead. I'm not into watching soap operas, but I think I learned more about two of the characters' plans to set up another character than I did about examining a comatose patient.
The one thing though that I did take away from this otherwise useless experience was a better understanding of why it is so difficult for physicians and family members to disconnect brain-dead patients from respirators and feeding tubes. Our patient was in a persistent vegetative state, but sometimes he would spontaneously open his eyes, start breathing harder as if he were gasping for air, and make other slight movements. Even though his higher brain function is completely gone, he does not respond in any way whatsoever to painful stimuli, and there is no chance that he will ever wake up, seeing him make those spontaneous movements gives the observer an impression like he's still aware on some level. I can only imagine if I felt that way how an emotional family member with no medical training and a fervent desire to have their loved one back would refuse to believe that this person could never wake up. As it turns out, this particular patient's family does not want to disconnect him from the respirator.
I didn't get a chance to do the reading for either seminar today, but it was ok because I was able to skim through the chapters during the seminars. The first seminar was about the vestibular system, and the seminar leader, although a nice guy and clearly trying to do his best, was way overambitious. He had 69 slides for a 50-minute seminar! Unsurprisingly, he had to deliver his talk at breakneck speed, and we ran way over. The second seminar was about hearing. It was given by two audiologists. I hadn't realized that any audiologists worked at CCF, but there are at least two. Audiologists treat patients with hearing or vestibular problems, but they aren't physicians. They have their own degree called a doctorate of audiology. These two audiologists were both really nice too, but their seminar had the opposite problem--it was kind of repetitive and not the most interesting.
In the afternoon, I had two clinical correlations. The first one was for doing neurological exams on patients with neuro disorders, and it was really great. We saw patients with Parkinson's disease (PD) and multiple sclerosis. One of the PD patients has a deep brain stimulator (DBS) implanted, and he turned it off for us so that we could see how bad his tremors were without it. DBS is incredibly cool technology and its use in PD is becoming more common. In a nutshell, the patient gets a sort of pacemaker implanted into an area of their brain called the globus pallidus. The neurons there are part of a movement pathway from another area called the substantia nigra, and neurons from the substantia nigra get destroyed in PD. The pathways are pretty complex, but the end result is a lack of volitional movement, and that's what DBS can help overcome. (If you're interested in DBS, you can read more about it here.)
The second clinical correlation wasn't very good, but apparently some of the other groups had a better experience. My group wound up waiting for half an hour at the desk in the neuro ICU. The secretary paged the doctor for us, and he said he would come get us, but no one ever came. So finally, we started wandering around the neuro ICU until we ran into another doc who took us in to see one of the comatose patients and went through the general procedure of how they examine these patients. We didn't get to actually examine the patient though, and I didn't really get much out of it. It was especially hard to concentrate on what the doctor was saying because the TV was blaring overhead. I'm not into watching soap operas, but I think I learned more about two of the characters' plans to set up another character than I did about examining a comatose patient.
The one thing though that I did take away from this otherwise useless experience was a better understanding of why it is so difficult for physicians and family members to disconnect brain-dead patients from respirators and feeding tubes. Our patient was in a persistent vegetative state, but sometimes he would spontaneously open his eyes, start breathing harder as if he were gasping for air, and make other slight movements. Even though his higher brain function is completely gone, he does not respond in any way whatsoever to painful stimuli, and there is no chance that he will ever wake up, seeing him make those spontaneous movements gives the observer an impression like he's still aware on some level. I can only imagine if I felt that way how an emotional family member with no medical training and a fervent desire to have their loved one back would refuse to believe that this person could never wake up. As it turns out, this particular patient's family does not want to disconnect him from the respirator.
Tuesday, November 06, 2007
All About Pain
I've spent the past two days learning about pain, thinking about pain, and reading about pain, but luckily not experiencing too much of it, at least not physically. Yesterday, we had a PBL case and a seminar that were both about pain, and today we had an anatomy session about the trigeminal system. The trigeminal nerve is one of the cranial nerves that innervates the face. (It's the fifth cranial nerve, if you were wondering.) As you can see in the picture, the trigeminal has three branches that go to the forehead, cheeks, and chin, and they all detect pain in the face among other things. 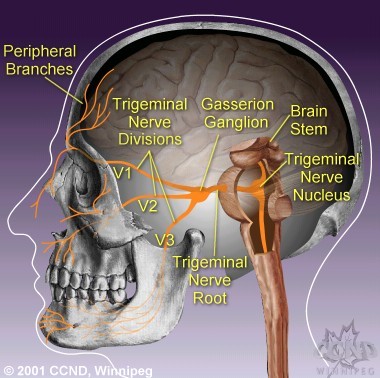 Pain is a very complex sense, because it has such a huge emotional component to it. If you're afraid of the pain, it can actually make your pain worse.
Pain is a very complex sense, because it has such a huge emotional component to it. If you're afraid of the pain, it can actually make your pain worse.
We had FCM this week, and it was about health care policy decisions. There were no small groups--we just had a speaker from the Case Business School for the full hour and a half. This same guy has spoken to us before. I think most of my classmates liked his talk, but I have to say that health care policy bores me to tears. It was, well, kind painful to sit through an hour and a half long lecture on it.
In clinic this afternoon, I had a patient who fit in with the whole pain theme perfectly--she has severe, chronic migraine headaches. There wasn't much for me to do about the migraines besides take the history because the patient was already being followed up at the CCF Pain Clinic. But still, we had quite a lengthy discussion about possible triggers, how the headaches affect her quality of life, and so on. I get an occasional headache myself every now and then, but nothing like this poor patient.
I meant to ask my preceptor today if patients who fit the topics we are covering in school are being booked this way on purpose. If not, this has to be the longest string of coincidences I've ever experienced. Or, maybe it's just that symptoms like pain and headaches are so ubiquitous and I haven't been keeping track of how many previous patients I've seen with headaches. Now that I think about it, patient complaints of headaches aren't exactly rare. If you go through the review of systems with a patient and ask them if they have this or that symptom, almost everyone will say yes to headaches. Who doesn't get a headache every now and then?
Pain is a very complex sense, because it has such a huge emotional component to it. If you're afraid of the pain, it can actually make your pain worse.We had FCM this week, and it was about health care policy decisions. There were no small groups--we just had a speaker from the Case Business School for the full hour and a half. This same guy has spoken to us before. I think most of my classmates liked his talk, but I have to say that health care policy bores me to tears. It was, well, kind painful to sit through an hour and a half long lecture on it.
In clinic this afternoon, I had a patient who fit in with the whole pain theme perfectly--she has severe, chronic migraine headaches. There wasn't much for me to do about the migraines besides take the history because the patient was already being followed up at the CCF Pain Clinic. But still, we had quite a lengthy discussion about possible triggers, how the headaches affect her quality of life, and so on. I get an occasional headache myself every now and then, but nothing like this poor patient.
I meant to ask my preceptor today if patients who fit the topics we are covering in school are being booked this way on purpose. If not, this has to be the longest string of coincidences I've ever experienced. Or, maybe it's just that symptoms like pain and headaches are so ubiquitous and I haven't been keeping track of how many previous patients I've seen with headaches. Now that I think about it, patient complaints of headaches aren't exactly rare. If you go through the review of systems with a patient and ask them if they have this or that symptom, almost everyone will say yes to headaches. Who doesn't get a headache every now and then?
Monday, November 05, 2007
Blogger Challenge Update
Yesterday, a very generous reader donated the remaining amount needed to fully fund the Mississippi skeleton project. I received a very nice letter from the teacher of this class, and I would like to post it here so that everyone who contributed to funding this project will know how much this teacher and her students appreciate what you've done for them.
Thank you so much! I cannot wait until school takes in on Monday to tell my students about your wonderful gift to them! They will be thrilled! Words cannot express the gratitude that I feel. The impact of your generosity will continue through the years to come, and I will make certain that my students remember that a stranger out there cared enough about them to make sure they got what they needed for their education. You will never know the boost to their esteem that such thing produces. Again, thank you from the bottom of my heart, and on behalf of my students, bless you!
I would like to again thank ALL of you generous readers who have donated to the CCLCM Student Blogger Challenge. At this point, we have raised a grand total of $494 to help low-income middle school students, and we have fully funded the Mississippi skeleton project. However, the Bronx reading project still needs another $401. If any of you have been thinking about donating but haven't gotten around to it yet, please consider giving a few dollars so that we can get those books to the kids.
Also, I was looking around on Donors Choose some more over the weekend, and there are so many great medicine and science-themed projects that need funding. I wish I could fund them all. If some of you readers are looking to make a tax-deductible contribution to charity before 2007 slips away from us, here are some other projects that caught my eye. The expiration date is the date when Donors Choose will remove that proposal from their website if it has not been fully funded by that point.
Concentrated Science Investigation (CSI) is a proposal to buy a set of forensics kits for inner city middle school children in North Carolina--expires April 27
First Step Lab, Second Step Nursing School is a proposal to buy two balances for use by low-income, pre-nursing high school students in rural Mississipi--expires April 29
Skeleton in the Classroom is a proposal to buy a model skeleton for inner city elementary school children in Texas--expires June 16
1-2-3..Bison To The Rescue! is a proposal to buy CPR kits to train low income high school students to administer CPR in rural Alabama--expires June 24
Inner Space - What a Trip! is a proposal to buy prepared microscope slides for low income middle school children in rural Mississippi--expires June 27
Protons, Neutrons, Electrons - Oh My! is a proposal to buy chemistry models of DNA and atoms for low income middle school children in rural Mississippi--expires June 27
Exploring The Human Body is a proposal to buy a model of the human body for low income elementary and middle school children in inner city Chicago--expires June 29
Inspiring Future (Urban) Doctors and Nurses is a proposal to buy dissecting supplies for inner city high school students in Massachussetts--expires June 30
Thank you so much! I cannot wait until school takes in on Monday to tell my students about your wonderful gift to them! They will be thrilled! Words cannot express the gratitude that I feel. The impact of your generosity will continue through the years to come, and I will make certain that my students remember that a stranger out there cared enough about them to make sure they got what they needed for their education. You will never know the boost to their esteem that such thing produces. Again, thank you from the bottom of my heart, and on behalf of my students, bless you!
I would like to again thank ALL of you generous readers who have donated to the CCLCM Student Blogger Challenge. At this point, we have raised a grand total of $494 to help low-income middle school students, and we have fully funded the Mississippi skeleton project. However, the Bronx reading project still needs another $401. If any of you have been thinking about donating but haven't gotten around to it yet, please consider giving a few dollars so that we can get those books to the kids.
Also, I was looking around on Donors Choose some more over the weekend, and there are so many great medicine and science-themed projects that need funding. I wish I could fund them all. If some of you readers are looking to make a tax-deductible contribution to charity before 2007 slips away from us, here are some other projects that caught my eye. The expiration date is the date when Donors Choose will remove that proposal from their website if it has not been fully funded by that point.
Concentrated Science Investigation (CSI) is a proposal to buy a set of forensics kits for inner city middle school children in North Carolina--expires April 27
First Step Lab, Second Step Nursing School is a proposal to buy two balances for use by low-income, pre-nursing high school students in rural Mississipi--expires April 29
Skeleton in the Classroom is a proposal to buy a model skeleton for inner city elementary school children in Texas--expires June 16
1-2-3..Bison To The Rescue! is a proposal to buy CPR kits to train low income high school students to administer CPR in rural Alabama--expires June 24
Inner Space - What a Trip! is a proposal to buy prepared microscope slides for low income middle school children in rural Mississippi--expires June 27
Protons, Neutrons, Electrons - Oh My! is a proposal to buy chemistry models of DNA and atoms for low income middle school children in rural Mississippi--expires June 27
Exploring The Human Body is a proposal to buy a model of the human body for low income elementary and middle school children in inner city Chicago--expires June 29
Inspiring Future (Urban) Doctors and Nurses is a proposal to buy dissecting supplies for inner city high school students in Massachussetts--expires June 30
Friday, November 02, 2007
Utterly Exhausted
I keep foolishly thinking that things are finally going to slow down at some point, but they never do. This week was the worst yet. I have only managed to get about half of the week's reading done, and I didn't get any reading done for my MS class yesterday at all. Obviously, this is not going to be a fun weekend, and next week is not looking much better, unfortunately.
This morning's seminars were on neuropsychology and gait disorders. The neuropsychologist who did the neuropsych session came last year also. She was showing us the tests that they give to people to see if they have dementia. Even though we had seen all of these tests last year, it was really helpful to see them again. Somehow, I am just getting more out of seeing these things this year. I think it's because now I'm only 95% confused about neuro instead of a complete 100%. The second session was with Dr. Chemali, who gave us a neuro session on sensation last year. He didn't play Celine Dion for us this year, but we reviewed all of the spinal pathways, and again, it seems to all just be making more sense.
Our ARM session today was a follow-up to last week's small group session where we are ostensibly supposed to be learning about how to write grants. It was, to put it kindly, completely useless. Each group was supposed to give a brief presentation about the project they had come up with, and I volunteered myself and one of my none-too-thrilled classmates to present for our group. The presentations went better than I had expected, because they actually did generate some discussion. But all in all, it was still a pointless exercise in terms of its stated purpose to teach us about writing grants. I think I mentioned last week that you would always start working on a grant by reading the literature so that you knew what the problems in that field are, which we didn't do. That's a pretty important step to just skip over! We were just coming up with hypotheses and methods out of thin air, which doesn't really give a very realistic simulation of the grant-writing experience. This exercise really should be made more structured, if not eliminated from the curriculum altogether.
This morning's seminars were on neuropsychology and gait disorders. The neuropsychologist who did the neuropsych session came last year also. She was showing us the tests that they give to people to see if they have dementia. Even though we had seen all of these tests last year, it was really helpful to see them again. Somehow, I am just getting more out of seeing these things this year. I think it's because now I'm only 95% confused about neuro instead of a complete 100%. The second session was with Dr. Chemali, who gave us a neuro session on sensation last year. He didn't play Celine Dion for us this year, but we reviewed all of the spinal pathways, and again, it seems to all just be making more sense.
Our ARM session today was a follow-up to last week's small group session where we are ostensibly supposed to be learning about how to write grants. It was, to put it kindly, completely useless. Each group was supposed to give a brief presentation about the project they had come up with, and I volunteered myself and one of my none-too-thrilled classmates to present for our group. The presentations went better than I had expected, because they actually did generate some discussion. But all in all, it was still a pointless exercise in terms of its stated purpose to teach us about writing grants. I think I mentioned last week that you would always start working on a grant by reading the literature so that you knew what the problems in that field are, which we didn't do. That's a pretty important step to just skip over! We were just coming up with hypotheses and methods out of thin air, which doesn't really give a very realistic simulation of the grant-writing experience. This exercise really should be made more structured, if not eliminated from the curriculum altogether.
Wednesday, October 31, 2007
Neuro Clinical Correlations
Today was another double seminar day. The first one was about the genetics of dementia, and for the second they showed us video clips of patients with various movement disorders. I liked the genetics seminar, which was a case with a sort of surprise conclusion. The other one was ok, but somehow I just couldn't keep focused. Maybe it's just a matter of it being the last hour of class and the room being nice and dark.
In the afternoon, we had two clinical correlations. The first one involved examining a patient with multiple sclerosis in small groups, which was interesting. But I felt sorry for the patient, who seemed to be pretty tired and kept dozing off in between getting various joints and muscles prodded and poked by us. Afterward, we got an hour-long seminar about MS, which wasn't bad, but it was too long. We had several questions for the speaker, and he had clearly not built in time for questions in his talk. So he started getting a little testy with us for asking so many questions, and we wound up arriving at the EMG lab about 20 minutes late.
EMG stands for electromyography, which is a fancy word for testing the electrical conduction in muscles. They asked us to volunteer for some of the tests, and I did one called a QSART where they administered acetylcholine (a neurotransmitter) to my skin and measured how much it made me sweat. This tests the small nerve fibers that are attached to the sweat glands. I am apparently a slow sweater, because we had to wait a few minutes before anything happened. It doesn't make you sweat gallons or anything--they just collected on the order of a nanoliter of sweat, which is 1 x 10^-9 liters. Two of my classmates did the other tests, one to test breathing and one to test pupillary reflexes. That pupillary one was really cool. We could see his eyes on the computer screen, and when the light flashed, his pupils would contract.
Afterward, we went to a second room to do nerve conduction studies. No one wanted to volunteer, so I did those too. First, they put two electrodes on my hand, and when they then applied a current, it made the muscle contract. That test looks to see if my nerve cells have lost their myelin in some segments. (Myelin is the "insulation" that covers your nerve cells.) It's kind of a weird feeling, because each time the tech turned on the current, my thumb would jerk, and I had no control over it whatsoever. It didn't really hurt though until they moved the current up to my elbow and made my whole arm move. That felt a lot like banging my funny bone, and it was not too pleasant. The second test involved sticking a needle into my thumb muscle. That test is to look for loss or degeneration of my nerve cell axons. The needle is really small, so it didn't really hurt, and the tech said my readings were normal for a young adult. What a relief!
In the afternoon, we had two clinical correlations. The first one involved examining a patient with multiple sclerosis in small groups, which was interesting. But I felt sorry for the patient, who seemed to be pretty tired and kept dozing off in between getting various joints and muscles prodded and poked by us. Afterward, we got an hour-long seminar about MS, which wasn't bad, but it was too long. We had several questions for the speaker, and he had clearly not built in time for questions in his talk. So he started getting a little testy with us for asking so many questions, and we wound up arriving at the EMG lab about 20 minutes late.
EMG stands for electromyography, which is a fancy word for testing the electrical conduction in muscles. They asked us to volunteer for some of the tests, and I did one called a QSART where they administered acetylcholine (a neurotransmitter) to my skin and measured how much it made me sweat. This tests the small nerve fibers that are attached to the sweat glands. I am apparently a slow sweater, because we had to wait a few minutes before anything happened. It doesn't make you sweat gallons or anything--they just collected on the order of a nanoliter of sweat, which is 1 x 10^-9 liters. Two of my classmates did the other tests, one to test breathing and one to test pupillary reflexes. That pupillary one was really cool. We could see his eyes on the computer screen, and when the light flashed, his pupils would contract.
Afterward, we went to a second room to do nerve conduction studies. No one wanted to volunteer, so I did those too. First, they put two electrodes on my hand, and when they then applied a current, it made the muscle contract. That test looks to see if my nerve cells have lost their myelin in some segments. (Myelin is the "insulation" that covers your nerve cells.) It's kind of a weird feeling, because each time the tech turned on the current, my thumb would jerk, and I had no control over it whatsoever. It didn't really hurt though until they moved the current up to my elbow and made my whole arm move. That felt a lot like banging my funny bone, and it was not too pleasant. The second test involved sticking a needle into my thumb muscle. That test is to look for loss or degeneration of my nerve cell axons. The needle is really small, so it didn't really hurt, and the tech said my readings were normal for a young adult. What a relief!
Tuesday, October 30, 2007
Officially Accepted to Grad School
So far, this week has been way intense. We are having double seminars every day again, and double reading too. Sigh. But the seminars have continued to be good on the whole. Yesterday we covered neurodegenerative diseases, and today we did inflammation and infection in the central nervous system. We also had a neuroanatomy session instead of FCM, which is both good and bad. It's good because it was more useful and interesting than an FCM seminar would have been, but it's bad because we had to read forty pages of neuroanatomy on top of all the reading for the other two seminars. Double sigh. My PBL learning objective for Wednesday is about the pathophysiology of tremors.
Clinic this afternoon was really busy. I saw five patients instead of the usual four. I don't know if my preceptor's secretary is scheduling certain patients this way on purpose, but it's uncanny how often I see a patient whose condition is related to whatever we're studying in school at the time. We're covering movement disorders like Parkinson's Disease and multiple sclerosis this week, and what do you know, I had an MS patient in clinic today. I did a neuro exam on the patient, not only because I need to practice doing the neuro exam, but also because there were actually some abnormal findings, mainly cerebellar (having to do with walking and balance). This morning, I also practiced doing some of the mini-mental status exam on one of the first years who had said he was worried about his mental faculties. He is not demented, at least as far as I got in testing him. ;-)
Finally, I am proud to say that I have officially been accepted to the Case Western Reserve University School of Graduate Studies. They sent me an official acceptance letter and everything. It's pretty funny actually, especially the second paragraph:
Dear CCLCMer,
Your credentials for admission to graduate study in the MS/MD program offered through the Clinical Research Scholars Program and the Cleveland Clinic Lerner College of Medicine have been reviewed. I am pleased to inform you that you have been retroactively admitted to this program with full standing for the term beginning August 27, 2007.
I regret that it will not be possible to provide you with an assistantship or fellowship. We have many more applicants for such appointments than we can provide, and our inability to offer you financial aid is no reflection on your promise as a graduate student.
I can't really complain about not getting financial aid. First of all, I didn't even know that I could apply for an assistantship, never mind actually applying for one. Second of all, I'm not actually paying for this MS because the grad classes are included in our med school tuition, so it would be pretty funny if the grad school started giving me financial aid too. All in all, I guess I just should be glad the grad school didn't decide that the med school had made a mistake two years ago when the med school admitted me! :-P
Clinic this afternoon was really busy. I saw five patients instead of the usual four. I don't know if my preceptor's secretary is scheduling certain patients this way on purpose, but it's uncanny how often I see a patient whose condition is related to whatever we're studying in school at the time. We're covering movement disorders like Parkinson's Disease and multiple sclerosis this week, and what do you know, I had an MS patient in clinic today. I did a neuro exam on the patient, not only because I need to practice doing the neuro exam, but also because there were actually some abnormal findings, mainly cerebellar (having to do with walking and balance). This morning, I also practiced doing some of the mini-mental status exam on one of the first years who had said he was worried about his mental faculties. He is not demented, at least as far as I got in testing him. ;-)
Finally, I am proud to say that I have officially been accepted to the Case Western Reserve University School of Graduate Studies. They sent me an official acceptance letter and everything. It's pretty funny actually, especially the second paragraph:
Dear CCLCMer,
Your credentials for admission to graduate study in the MS/MD program offered through the Clinical Research Scholars Program and the Cleveland Clinic Lerner College of Medicine have been reviewed. I am pleased to inform you that you have been retroactively admitted to this program with full standing for the term beginning August 27, 2007.
I regret that it will not be possible to provide you with an assistantship or fellowship. We have many more applicants for such appointments than we can provide, and our inability to offer you financial aid is no reflection on your promise as a graduate student.
I can't really complain about not getting financial aid. First of all, I didn't even know that I could apply for an assistantship, never mind actually applying for one. Second of all, I'm not actually paying for this MS because the grad classes are included in our med school tuition, so it would be pretty funny if the grad school started giving me financial aid too. All in all, I guess I just should be glad the grad school didn't decide that the med school had made a mistake two years ago when the med school admitted me! :-P
Friday, October 26, 2007
Already Sick of Step I
I forgot to mention on Wednesday that you should never tangle with a psychiatrist, because they will always get the last word. When Dean Franco was giving one of our coma seminars, I asked her how she could tell if the patient actually wasn't paying attention due to delirium versus for some other reason. She said if they weren't paying attention for any reason, then it was an alteration of consciousness. So I said, "No, I mean, what if you're asking me where I am or the date, and I just don't want to answer your questions?" Much to the amusement of my classmates, she replied, "Then it means you have a personality disorder!"
Yesterday wasn't terribly eventful. I had my MS class in the morning, though it was kind of hard to get up, and I spent the rest of the day working on my learning objective and trying to catch up on some reading.
Today we had a really good PBL session, probably one of the best we've done all block. The learning objectives were good, and the discussion was good. But no one from the administration came today to see us! Our seminars were on brain trauma and brain tumors. They were good too. I can't believe how much more I'm enjoying neuro this year versus last year. I don't know if the seminars are really just that much better, or the pathology is just more interesting, or I'm just feeling more comfortable with the material because of having studied neuro over the summer, or what.
Our ARM session today was, to put it mildly, simply awful. The school has decided to have us do little research projects where we come up with hypotheses and objectives and who knows what else at various points throughout the year, and today was the first one of those sessions. So we met in our PBL groups, and we were supposed to come up with an experiment based on our PBL case from this week. That has to be the most ridiculous way to come up with a research idea that I've ever heard. If you're wanting to come up with a research project and write a grant proposal, you don't start by thinking up methodology and making up a hypothesis! You start by reading the literature in that area so that you even understand what the current issues are in that field! On the bright side, I have a whole week to think of a way to give constructive criticism about this before we fill out the feedback sheet next Friday at the end of PBL. :-P
Dr. Prayson, who is a neuropathologist and also our new Assistant Dean of Students, invited anyone who was interested to go over the the CCF morgue and look at some brain pathology. About ten of us went this afternoon, and it was really awesome. We saw tumors, infarcts, hemorrhages, all kinds of interesting stuff that we had been learning about this week. One of the brains belonged to a young child, which was a little sad though. But overall, I got so much out of it in terms of learning the anatomy and pathology that I asked him about coming in to see an autopsy some time. He said that we were definitely welcome to do that if we wanted, and that some of the upperclassmen had done it in previous years. I don't know when I will have time to go, and it's kind of hard to set up a time anyway because patients don't exactly die and require autopsies on a set schedule. Maybe I can do it this summer after I take Step I.
Speaking of which, we got an email earlier in the week about attending a session this evening by some of the upperclassmen to give us advice on preparing for Step I. It was from 5:15-6:45 today. Although I felt kind of bad because of how nice the third and fourth years were to do this for us, I decided not to go. I was just too tired, and I also have come to realize that I really don't want to hear a single thing more about Step I at this point. It's bad enough that we have to register for it now, in October, when we aren't even taking it for another eight months. (The reason why we have to register now is that the Case UP students take the test four months earlier than we do, at the beginning of March.) But it's making me feel more stressed and anxious to be talking about studying for it now, when I don't have time to study for it and when I haven't learned enough path yet to even make it worth studying for it. I'm planning to start studying in January, and I don't want to think about it any more between now and then. Please, just give me my last two months of USMLE ignorant bliss!
For those of you who are premeds, don't complain about how much the MCAT costs, because the registration fee for Step I will set you back a cool $480, and Step II is even worse. For those of you who are CCLCM first years, start saving up. I didn't realize that we were going to have to register this early, right before the holidays, and I did not budget that $480 for this semester. :-(
Yesterday wasn't terribly eventful. I had my MS class in the morning, though it was kind of hard to get up, and I spent the rest of the day working on my learning objective and trying to catch up on some reading.
Today we had a really good PBL session, probably one of the best we've done all block. The learning objectives were good, and the discussion was good. But no one from the administration came today to see us! Our seminars were on brain trauma and brain tumors. They were good too. I can't believe how much more I'm enjoying neuro this year versus last year. I don't know if the seminars are really just that much better, or the pathology is just more interesting, or I'm just feeling more comfortable with the material because of having studied neuro over the summer, or what.
Our ARM session today was, to put it mildly, simply awful. The school has decided to have us do little research projects where we come up with hypotheses and objectives and who knows what else at various points throughout the year, and today was the first one of those sessions. So we met in our PBL groups, and we were supposed to come up with an experiment based on our PBL case from this week. That has to be the most ridiculous way to come up with a research idea that I've ever heard. If you're wanting to come up with a research project and write a grant proposal, you don't start by thinking up methodology and making up a hypothesis! You start by reading the literature in that area so that you even understand what the current issues are in that field! On the bright side, I have a whole week to think of a way to give constructive criticism about this before we fill out the feedback sheet next Friday at the end of PBL. :-P
Dr. Prayson, who is a neuropathologist and also our new Assistant Dean of Students, invited anyone who was interested to go over the the CCF morgue and look at some brain pathology. About ten of us went this afternoon, and it was really awesome. We saw tumors, infarcts, hemorrhages, all kinds of interesting stuff that we had been learning about this week. One of the brains belonged to a young child, which was a little sad though. But overall, I got so much out of it in terms of learning the anatomy and pathology that I asked him about coming in to see an autopsy some time. He said that we were definitely welcome to do that if we wanted, and that some of the upperclassmen had done it in previous years. I don't know when I will have time to go, and it's kind of hard to set up a time anyway because patients don't exactly die and require autopsies on a set schedule. Maybe I can do it this summer after I take Step I.
Speaking of which, we got an email earlier in the week about attending a session this evening by some of the upperclassmen to give us advice on preparing for Step I. It was from 5:15-6:45 today. Although I felt kind of bad because of how nice the third and fourth years were to do this for us, I decided not to go. I was just too tired, and I also have come to realize that I really don't want to hear a single thing more about Step I at this point. It's bad enough that we have to register for it now, in October, when we aren't even taking it for another eight months. (The reason why we have to register now is that the Case UP students take the test four months earlier than we do, at the beginning of March.) But it's making me feel more stressed and anxious to be talking about studying for it now, when I don't have time to study for it and when I haven't learned enough path yet to even make it worth studying for it. I'm planning to start studying in January, and I don't want to think about it any more between now and then. Please, just give me my last two months of USMLE ignorant bliss!
For those of you who are premeds, don't complain about how much the MCAT costs, because the registration fee for Step I will set you back a cool $480, and Step II is even worse. For those of you who are CCLCM first years, start saving up. I didn't realize that we were going to have to register this early, right before the holidays, and I did not budget that $480 for this semester. :-(
Wednesday, October 24, 2007
Crazy Daze
This week is just absolutely killing me, although today was a pretty good day as far as school goes. Our PBL group was being observed by one of the administration people this morning. I don't know what it is about us being watched, but somehow it does something to the group dynamics and makes us all act even weirder than we usually do. :-P My learning objective for Friday is on reading EEGs. Our seminars this morning were both about coma, and they were really good. I have to say that overall, this year's NMS block is vastly better than last year's was.
In the afternoon, I had my clinical skills course. First, we had to practice interviewing standardized patients about their sexual history. Most of it is pretty straightforward, but some of the examples we had to read were a little ridiculous. For example, there was one where the patient was arthritic, and the doctor asked if the patient could open their legs to have sex. I read that one and thought, there is no way I will ever ask any arthritic patient that question! Do I look like Dr. Kinsey or Dr. Ruth? I came here to be a clinical researcher, not a sex therapist!
The standardized patients were awesome though. The one I had was playing a lesbian with a rash on her groin, and the interview was pretty uneventful. I asked her about her sexual activity, partners, using protection, satisfaction with her sex life, if anyone was hurting her or forcing her to do anything she didn't want to do, etc. Some of my classmates apparently got treated to detailed descriptions of lesbian sex toys, but I didn't really give my actress too much of an opportunity to go into a lot of details. :-P It felt a lot more awkward doing the interview in class than it ever does in clinic. Having an audience of a physician, a shrink, and three of your classmates watching you interview this person on what is probably the most sensitive subject out there is kind of weird, even though it's all pretend. We got through it all right, but no one ever said that being professional all the time is easy. ;-)
Afterward, we had a Clinical Correlation on impaired physicians, which was AWESOME. Several physicians and nurses who were recovering addicts came to speak with us in small groups about their experiences. Most had been alcoholics, but some had been addicted to opioids or other drugs. They answered our questions about how their addiction had affected their professional and personal lives, and we talked about Alcoholics Anonymous as well. Some of these people attend AA or NA (Narcotics Anonymous) meetings every single day, up to four meetings per day. The main things I learned from this were that being isolated from others and feeling like they were "in control" were two of the biggest risk factors for becoming an addict, or relapsing after getting clean. They also mentioned that statistically, odds are that three or four people in my class of 32 will become addicts or have problems with alcohol or other drugs. That really made their stories seem even more pertinent to us.
This evening, I came home and wrote my paper for class tomorrow. It wound up taking about three and a half hours. I don't like writing papers at the last minute, and I am just so happy that I got it done in time, even though I didn't have a chance to do any of my reading for med school this evening. I can't do it now either, because my class is at 7 AM tomorrow. Sigh.
In the afternoon, I had my clinical skills course. First, we had to practice interviewing standardized patients about their sexual history. Most of it is pretty straightforward, but some of the examples we had to read were a little ridiculous. For example, there was one where the patient was arthritic, and the doctor asked if the patient could open their legs to have sex. I read that one and thought, there is no way I will ever ask any arthritic patient that question! Do I look like Dr. Kinsey or Dr. Ruth? I came here to be a clinical researcher, not a sex therapist!
The standardized patients were awesome though. The one I had was playing a lesbian with a rash on her groin, and the interview was pretty uneventful. I asked her about her sexual activity, partners, using protection, satisfaction with her sex life, if anyone was hurting her or forcing her to do anything she didn't want to do, etc. Some of my classmates apparently got treated to detailed descriptions of lesbian sex toys, but I didn't really give my actress too much of an opportunity to go into a lot of details. :-P It felt a lot more awkward doing the interview in class than it ever does in clinic. Having an audience of a physician, a shrink, and three of your classmates watching you interview this person on what is probably the most sensitive subject out there is kind of weird, even though it's all pretend. We got through it all right, but no one ever said that being professional all the time is easy. ;-)
Afterward, we had a Clinical Correlation on impaired physicians, which was AWESOME. Several physicians and nurses who were recovering addicts came to speak with us in small groups about their experiences. Most had been alcoholics, but some had been addicted to opioids or other drugs. They answered our questions about how their addiction had affected their professional and personal lives, and we talked about Alcoholics Anonymous as well. Some of these people attend AA or NA (Narcotics Anonymous) meetings every single day, up to four meetings per day. The main things I learned from this were that being isolated from others and feeling like they were "in control" were two of the biggest risk factors for becoming an addict, or relapsing after getting clean. They also mentioned that statistically, odds are that three or four people in my class of 32 will become addicts or have problems with alcohol or other drugs. That really made their stories seem even more pertinent to us.
This evening, I came home and wrote my paper for class tomorrow. It wound up taking about three and a half hours. I don't like writing papers at the last minute, and I am just so happy that I got it done in time, even though I didn't have a chance to do any of my reading for med school this evening. I can't do it now either, because my class is at 7 AM tomorrow. Sigh.
Tuesday, October 23, 2007
Round Two of Neuro Block
I had a lot of work to catch up on from last week over the weekend, which meant that I spent most of a very beautiful fall weekend indoors reading about addiction. It didn't quite drive me to drink, and maybe there's a future career for me here, because I actually got all of the SAQs right. (The SAQs are those multiple guess questions we have to do each week.) I have never done that before. The less good part is that I didn't really have much chance to do this week's reading, which means I am as much behind so far this week as ever. Plus, I have a paper due for my MS class on Thursday, so it's not going to be an easy week.
Monday we started our new PBL case, and the patient is in a coma. That is our theme for this week in general. The neuro faculty have been doubling up on the seminars, where we have two one-hour seminars instead of one two-hour seminar each day. The bad thing about that is that they're also assigning us double the reading in a lot of cases. The seminars have been very good though. Yesterday's were on the anatomy and pathology of stroke. The other good thing is that the readings overlap in topic quite a bit, so I am not totally lost in class even though I've been coming in having only finished half of the assigned reading for each seminar.
Today we had a neuroanatomy session. Like last time, they divided us into two groups. One part reviewed the vasculature and ventricles of the brain using models and preserved brains, and the other was a series of questions and cases. The FCM session afterward was about surrogate decision making, which we had already talked about once last year. It wasn't the greatest FCM session, but it wasn't absolutely horrible either.
I had clinic this afternoon, and it wound up being a busy day. The most interesting patient I saw was a guy who was in for a follow-up for hypertension. That didn't sound too exciting initially. But while I was taking his history, he was telling me about his life. It turned out that he was a retired garbage collector. He never went to high school, and after he retired he decided to start taking GED classes. He is old enough to be most of his classmates' father or even grandfather, but he said he was determined to pass the test and earn a high school diploma. I thought that was incredibly impressive and inspiring. When I presented his history afterward, I was amazed to learn that my preceptor, who has cared for this man for several years, never knew that he only had an eighth grade education or that he was working on earning a GED. My preceptor commented that it was common for doctors to just hand printed instructions to patients without ever considering that some patients might not be able to read them. This just proves the point that not obtaining a patient's education level and occupation as part of the history really can affect the doctor's ability to provide the best possible care for that patient.
Monday we started our new PBL case, and the patient is in a coma. That is our theme for this week in general. The neuro faculty have been doubling up on the seminars, where we have two one-hour seminars instead of one two-hour seminar each day. The bad thing about that is that they're also assigning us double the reading in a lot of cases. The seminars have been very good though. Yesterday's were on the anatomy and pathology of stroke. The other good thing is that the readings overlap in topic quite a bit, so I am not totally lost in class even though I've been coming in having only finished half of the assigned reading for each seminar.
Today we had a neuroanatomy session. Like last time, they divided us into two groups. One part reviewed the vasculature and ventricles of the brain using models and preserved brains, and the other was a series of questions and cases. The FCM session afterward was about surrogate decision making, which we had already talked about once last year. It wasn't the greatest FCM session, but it wasn't absolutely horrible either.
I had clinic this afternoon, and it wound up being a busy day. The most interesting patient I saw was a guy who was in for a follow-up for hypertension. That didn't sound too exciting initially. But while I was taking his history, he was telling me about his life. It turned out that he was a retired garbage collector. He never went to high school, and after he retired he decided to start taking GED classes. He is old enough to be most of his classmates' father or even grandfather, but he said he was determined to pass the test and earn a high school diploma. I thought that was incredibly impressive and inspiring. When I presented his history afterward, I was amazed to learn that my preceptor, who has cared for this man for several years, never knew that he only had an eighth grade education or that he was working on earning a GED. My preceptor commented that it was common for doctors to just hand printed instructions to patients without ever considering that some patients might not be able to read them. This just proves the point that not obtaining a patient's education level and occupation as part of the history really can affect the doctor's ability to provide the best possible care for that patient.
Friday, October 19, 2007
Back to School
I got home last night from my conference. It was really good, but also really exhausting. I have come to the realization that it is not very much fun to go to a conference as a second year medical student in the middle of an organ system block. The thing is, the psych profs are not giving me any extensions to turn my work in late or anything, so I had to spend several hours every morning and evening doing my reading and homework for school while all of the residents and fellows were going out having fun and sightseeing. I did manage to do a bit of sightseeing myself, but I definitely didn't have anywhere near as much fun as everyone else did. On the funny side, my PI commented to me that he was glad I came because I probably learned more at the meeting than I would have learned if I had stayed in Cleveland. I said I knew that I had definitely learned more than I would have otherwise, because I still had to do all of the assignments for school anyway, PLUS I attended a bunch of talks at the meeting. :-P
This morning we had PBL. I had been reading the case from the conference and had emailed some ideas and articles to the other members of my group, so I had a clue about what was going on even though I missed Monday and Wednesday. We have decided to be more organized and start having someone be the official board scribe each week. We also agreed that we would go back to doing formal learning objectives from now on.
The seminar today was about personality disorders. It's really funny, but as I was reading about the personality disorders yesterday and listening to the seminar today, I couldn't help but think about all of the people I have met in my life who would fit into one or another personality disorder category. I think probably everyone does this, but it was funny how many people I could say to myself, "hmm, yeah, he IS kind of borderline personality with features of anti-social personality." Yesterday on the plane, this surfer dude was sitting next to me. He saw the article I was reading about personality disorders for today's class and said that probably several of the categories would apply to him. I told him not to worry, substance abuse wasn't a personality disorder. He just kind of looked at me, so then I had to explain about the DSM axes and that personality disorders were a completely different category than being a pothead. Once he understood that he doesn't have a personality disorder (Axis II) because substance abuse is lumped in Axis I with things like psychotic disorders and dementia, he said, "oh, good, I'm really glad I'm not crazy." It made for a rather interesting conversation until he finally passed out after downing his third or fourth gin and tonic.
Our ARM seminar today was kind of boring, and I had a hard time focusing and paying attention the whole time. It was supposed to be about addiction, but instead it was about how some variant of the GABA ion channel seems to cause epilepsy in rats who were irradiated in the womb. Besides the fact that it's kind of cruel to irradiate pregnant rats, I'm not sure how well this rat model even mimics the human disease. The speaker did do studies on human tissue from epileptic patients as well, but he used "non-epileptic" tissue from these same patients as his controls. I wonder if non-epileptic tissue from epileptic patients is actually equivalent to normal brain tissue from non-epileptic patients? It's not like you could take some brain tissue out of a normal person and find out!
This morning we had PBL. I had been reading the case from the conference and had emailed some ideas and articles to the other members of my group, so I had a clue about what was going on even though I missed Monday and Wednesday. We have decided to be more organized and start having someone be the official board scribe each week. We also agreed that we would go back to doing formal learning objectives from now on.
The seminar today was about personality disorders. It's really funny, but as I was reading about the personality disorders yesterday and listening to the seminar today, I couldn't help but think about all of the people I have met in my life who would fit into one or another personality disorder category. I think probably everyone does this, but it was funny how many people I could say to myself, "hmm, yeah, he IS kind of borderline personality with features of anti-social personality." Yesterday on the plane, this surfer dude was sitting next to me. He saw the article I was reading about personality disorders for today's class and said that probably several of the categories would apply to him. I told him not to worry, substance abuse wasn't a personality disorder. He just kind of looked at me, so then I had to explain about the DSM axes and that personality disorders were a completely different category than being a pothead. Once he understood that he doesn't have a personality disorder (Axis II) because substance abuse is lumped in Axis I with things like psychotic disorders and dementia, he said, "oh, good, I'm really glad I'm not crazy." It made for a rather interesting conversation until he finally passed out after downing his third or fourth gin and tonic.
Our ARM seminar today was kind of boring, and I had a hard time focusing and paying attention the whole time. It was supposed to be about addiction, but instead it was about how some variant of the GABA ion channel seems to cause epilepsy in rats who were irradiated in the womb. Besides the fact that it's kind of cruel to irradiate pregnant rats, I'm not sure how well this rat model even mimics the human disease. The speaker did do studies on human tissue from epileptic patients as well, but he used "non-epileptic" tissue from these same patients as his controls. I wonder if non-epileptic tissue from epileptic patients is actually equivalent to normal brain tissue from non-epileptic patients? It's not like you could take some brain tissue out of a normal person and find out!
Friday, October 12, 2007
End of a Hectic Week
I'm leaving for my conference tomorrow! I just finished packing my suitcase, including my suit, which I haven't worn since I was interviewing for medical school two years ago. :-P The entire week has just been so crazy because I had to do this week's school work, get prepared for the conference, and collect up next week's assignments to take with me.
One of next week's assignments is for us to attend an Alcoholics Anonymous (AA) meeting. I went to one at a church near CCF after my MS class yesterday morning with two of my classmates. It was a very good experience, much better than I could have possibly anticipated. We met some regulars who have been coming to AA meetings for several decades. Others were first-time attendees like we were. We told the AA members that we are medical students at the Clinic, we are studying addiction and alcoholism in school, and we want to learn more about how to help our alcoholic patients beat their addiction. I wasn't sure how the regulars would feel about us coming, but they seemed happy to have us there. Several of them even came up to us afterward and talked to us more about their lives, and they invited us to come back again for another meeting whenever we wanted.
Yesterday was just a whirlwind. After the AA meeting, I got my PBL evals finished since they were due today, and I finished logging in all of my patients from Wednesday's peds clinic. It turns out that I saw EIGHT patients. No wonder I was so exhausted--that's twice as many as I see on a normal clinic day in IM! I also prepared my PBL learning objective, which was on adolescent depression.
Our seminar this morning was about sleep, and within a few minutes after it began, I was very tempted to go to sleep. Good thing that 3-57 (the library room where we have our classes) is so cold, or I really might have fallen asleep. The ARM (almost called it POD again!) talk today was kind of boring too. It was about preventing the blood vessels over the brain from spasming and leading to stroke in patients who have just had an aneurysm in the brain. That is an interesting topic, but for some reason the session turned into a discussion between the speaker and the professor in charge of the seminar series. Last year, the prof in charge hardly ever spoke, because the sessions are supposed to be for the students to interact with the faculty, not for the faculty to interact with each other. Not very cool.
There was a neuro histology review session this afternoon. But it was optional, so I opted not to go. Neuro histology wasn't so interesting the first time around that I wanted to go through it again, and I had enough other stuff to do.
I want to take the time to thank those of you who have donated to my Blogger Challenge this past week. So far we have raised $83 toward our goal of $951 to buy a skeleton model and books for underprivileged middle school children. If any of you other readers would like to find out more about my Blogger Challenge or help out, please click here.
One of next week's assignments is for us to attend an Alcoholics Anonymous (AA) meeting. I went to one at a church near CCF after my MS class yesterday morning with two of my classmates. It was a very good experience, much better than I could have possibly anticipated. We met some regulars who have been coming to AA meetings for several decades. Others were first-time attendees like we were. We told the AA members that we are medical students at the Clinic, we are studying addiction and alcoholism in school, and we want to learn more about how to help our alcoholic patients beat their addiction. I wasn't sure how the regulars would feel about us coming, but they seemed happy to have us there. Several of them even came up to us afterward and talked to us more about their lives, and they invited us to come back again for another meeting whenever we wanted.
Yesterday was just a whirlwind. After the AA meeting, I got my PBL evals finished since they were due today, and I finished logging in all of my patients from Wednesday's peds clinic. It turns out that I saw EIGHT patients. No wonder I was so exhausted--that's twice as many as I see on a normal clinic day in IM! I also prepared my PBL learning objective, which was on adolescent depression.
Our seminar this morning was about sleep, and within a few minutes after it began, I was very tempted to go to sleep. Good thing that 3-57 (the library room where we have our classes) is so cold, or I really might have fallen asleep. The ARM (almost called it POD again!) talk today was kind of boring too. It was about preventing the blood vessels over the brain from spasming and leading to stroke in patients who have just had an aneurysm in the brain. That is an interesting topic, but for some reason the session turned into a discussion between the speaker and the professor in charge of the seminar series. Last year, the prof in charge hardly ever spoke, because the sessions are supposed to be for the students to interact with the faculty, not for the faculty to interact with each other. Not very cool.
There was a neuro histology review session this afternoon. But it was optional, so I opted not to go. Neuro histology wasn't so interesting the first time around that I wanted to go through it again, and I had enough other stuff to do.
I want to take the time to thank those of you who have donated to my Blogger Challenge this past week. So far we have raised $83 toward our goal of $951 to buy a skeleton model and books for underprivileged middle school children. If any of you other readers would like to find out more about my Blogger Challenge or help out, please click here.
Wednesday, October 10, 2007
Adolescent Medicine
We had PBL and a seminar on bipolar disorders this morning. The seminar wound up being pretty good, even though the speaker basically didn't cover anticonvulsant drugs at all like he was supposed to do.
In the afternoon, I had peds clinic. I was working with an adolescent medicine specialist. I went in there thinking, "Oh, great, yet another exciting afternoon of well child visits." I figured maybe if I was lucky there would be a few sore throats or earaches. But this clinic was awesome, probably the best clinic day I've ever had. My patients were all teens, and most of them had eating disorders. One was also hearing voices. They were a lot like the kid we've been reading about in this week's PBL case. I know everyone has their share of teenage angst, but not like this. These patients really need help. It was incredibly interesting and also very sad to hear their stories and how much they suffer with body image issues and other problems. I definitely identified with several of them. One patient in particular wanted to go to medical school and even knew all about CCLCM.
I was utterly exhausted by the end of the afternoon. I think today was a lot more emotional for me since I was seeing teens. It was really intense and fast-paced and just an all-around great experience. I am doing my next peds clinic with this same doctor. I'm really not all that interested in going into peds. But if I did do peds, I'd definitely do adolescent medicine!
In the afternoon, I had peds clinic. I was working with an adolescent medicine specialist. I went in there thinking, "Oh, great, yet another exciting afternoon of well child visits." I figured maybe if I was lucky there would be a few sore throats or earaches. But this clinic was awesome, probably the best clinic day I've ever had. My patients were all teens, and most of them had eating disorders. One was also hearing voices. They were a lot like the kid we've been reading about in this week's PBL case. I know everyone has their share of teenage angst, but not like this. These patients really need help. It was incredibly interesting and also very sad to hear their stories and how much they suffer with body image issues and other problems. I definitely identified with several of them. One patient in particular wanted to go to medical school and even knew all about CCLCM.
I was utterly exhausted by the end of the afternoon. I think today was a lot more emotional for me since I was seeing teens. It was really intense and fast-paced and just an all-around great experience. I am doing my next peds clinic with this same doctor. I'm really not all that interested in going into peds. But if I did do peds, I'd definitely do adolescent medicine!
Tuesday, October 09, 2007
Classes and Clinic
Our PBL case this week is pretty interesting, particularly because it keeps getting more complicated and taking unexpected turns. Also, we are supposed to be meeting a patient who has the disease the patient in the PBL case has after Friday's session. Yesterday's seminar was given jointly by a psychiatrist and a psychologist. It was ok, but they could have made it more detailed. I don't know if it's just me, but sometimes it seems like the psych people spend an awful lot of time justifying their field and the work they do. The only other interesting thing that happened yesterday is that I submitted my poster to the CCF art department for printing after class. It will be ready for Friday.
This morning, we had an anatomy session covering neuropsych. The first half went over pictures from our book, and we were asked to locate structures on drawings and brain models for the second half. I only got about a third of the reading done in time for today's session because for some reason, the assignment didn't get put up on the portal until yesterday afternoon. I really hate when they give us the assignments last minute like that. I had actually been more or less keeping up with the reading so far this block until today. :-P
The FCM session was about professionalism, and my small group had a pretty interesting discussion about what to do with patients you just don't like, or patients who you feel you really can't help. The large group talk was all about the life of William Osler, and I should have just skipped it.
My clinic preceptor's secretary forgot to email me to let me know that my preceptor wouldn't be in clinic today. So when I showed up clueless, one of the nurses told me I could just go home. But I didn't want to skip clinic this week since I won't be doing any clinic next week and we are only allowed to miss three or four sessions all year. (I want to wait and miss them in May when I am studying for the boards, not in October!)
I wound up working with a resident and his preceptor instead. We saw three patients. One had a sexually transmitted disease, and oh boy, I'm glad that I am not the one who has to break the news to someone that their spouse was probably fooling around on them. Another one had a rheumatological condition, so that was good timing after last week. The resident and I did a neurological and musculoskeletal exam on the patient. We wound up spending a lot of time in the room with that patient, but it was a good learning experience, and I think we really made the patient feel a lot better. Sometimes just having a name for whatever is wrong with you makes it easier for you to bear having a disease, and that was definitely true in this patient's case.
This morning, we had an anatomy session covering neuropsych. The first half went over pictures from our book, and we were asked to locate structures on drawings and brain models for the second half. I only got about a third of the reading done in time for today's session because for some reason, the assignment didn't get put up on the portal until yesterday afternoon. I really hate when they give us the assignments last minute like that. I had actually been more or less keeping up with the reading so far this block until today. :-P
The FCM session was about professionalism, and my small group had a pretty interesting discussion about what to do with patients you just don't like, or patients who you feel you really can't help. The large group talk was all about the life of William Osler, and I should have just skipped it.
My clinic preceptor's secretary forgot to email me to let me know that my preceptor wouldn't be in clinic today. So when I showed up clueless, one of the nurses told me I could just go home. But I didn't want to skip clinic this week since I won't be doing any clinic next week and we are only allowed to miss three or four sessions all year. (I want to wait and miss them in May when I am studying for the boards, not in October!)
I wound up working with a resident and his preceptor instead. We saw three patients. One had a sexually transmitted disease, and oh boy, I'm glad that I am not the one who has to break the news to someone that their spouse was probably fooling around on them. Another one had a rheumatological condition, so that was good timing after last week. The resident and I did a neurological and musculoskeletal exam on the patient. We wound up spending a lot of time in the room with that patient, but it was a good learning experience, and I think we really made the patient feel a lot better. Sometimes just having a name for whatever is wrong with you makes it easier for you to bear having a disease, and that was definitely true in this patient's case.
Saturday, October 06, 2007
Please Support My Blogger Challenge!
This month, Blogger is partnering with DonorsChoose and asking blog authors to sponsor challenges to raise money for schools. Teachers at schools around the country are able to submit proposals, which are then verified and posted by the DonorsChoose staff. I would like to support two projects that are particularly meaningful to me as a medical student going to a school in an underserved area.
The first project is proposed by a teacher in the South Bronx. She is trying to raise money to buy books for her inner city middle school students to help inspire them to do something big with their lives. The book, which is based on a true story, is called "We Beat the Street." It describes how three boys went from being underprivileged teens to practicing physicians. Even today, there is a shortage of physicians working with minority and low-income populations. Therefore, I am asking my blog readers to please help inspire this teacher's students to think about medicine as a career goal. The total amount of money needed to buy books for all of the students is $536.
The second project is proposed by a science teacher in rural Mississippi. She would like to buy a skeleton model to teach her low income middle school students about human anatomy. She has almost no supplies to use to teach science to her students. I don't know if she will be able to spark an interest in any of them to become future physicians, but I'd like her to at least have the chance to try. She needs $421 to buy the skeleton model.
Thanks so much to those of you who are able to contribute. Even if you can only give a few dollars, every little bit will help. Please click here or on the icon below if you would like to donate to either project in this challenge. To see how much progress has been made toward reaching the total challenge goal of $896 to fund both projects, you can also check out the thermometer in the side bar.

The first project is proposed by a teacher in the South Bronx. She is trying to raise money to buy books for her inner city middle school students to help inspire them to do something big with their lives. The book, which is based on a true story, is called "We Beat the Street." It describes how three boys went from being underprivileged teens to practicing physicians. Even today, there is a shortage of physicians working with minority and low-income populations. Therefore, I am asking my blog readers to please help inspire this teacher's students to think about medicine as a career goal. The total amount of money needed to buy books for all of the students is $536.
The second project is proposed by a science teacher in rural Mississippi. She would like to buy a skeleton model to teach her low income middle school students about human anatomy. She has almost no supplies to use to teach science to her students. I don't know if she will be able to spark an interest in any of them to become future physicians, but I'd like her to at least have the chance to try. She needs $421 to buy the skeleton model.
Thanks so much to those of you who are able to contribute. Even if you can only give a few dollars, every little bit will help. Please click here or on the icon below if you would like to donate to either project in this challenge. To see how much progress has been made toward reaching the total challenge goal of $896 to fund both projects, you can also check out the thermometer in the side bar.
Friday, October 05, 2007
MS Class, Working on My Poster, Finishing Bones, and CCLCM Book Club
Yesterday's clinical trials class was again a review of stuff we had already learned over the summer and last semester. I'm not complaining though--at least one thing in my life is easy! I spent yesterday afternoon working on my poster, and unfortunately my preceptor is making me change things all around yet again. So I'll be doing that this weekend. Thankfully this will have to be the last round of revisions, because I have to turn it in to be printed on Monday.
This morning after PBL, we had two pharm seminars on treatments for rheumatological diseases. To say that the first seminar was poor is about as generous and kind as I can possibly be about it. Maybe that seminar leader was asked at the last minute to replace whoever was supposed to be giving the seminar, because I can't think of any other reason why someone would be that unprepared. The second seminar leader was considerably better. Our POD (oops, I mean ARM) talk today was a basic science one about several proteins involved in the vasculitis immune response. I was initially feeling wary of an entire hour-long talk that was chock-full of pictures of gels and immunoprecipitations, but it actually turned out to be pretty interesting. The speaker had given one of the POD seminars last year too, and this one was completely different.
In the evening, I went to the very first meeting of the new CCLCM Book Club. We had read "Better" by Atul Gawande. I was feeling really tired and cranky, and I almost didn't go. But in the end, I'm glad that I did go, because it was a lot of fun. One of the things that I liked best about it is that we had a mix of first, second, and third years. I had never thought about this, but having people from different classes meet to discuss ethical issues is a really great way to get a lot of different perspectives. I don't think it would work so well for PBL, but it might be useful to have some mixed-class FCM small group discussions.
This morning after PBL, we had two pharm seminars on treatments for rheumatological diseases. To say that the first seminar was poor is about as generous and kind as I can possibly be about it. Maybe that seminar leader was asked at the last minute to replace whoever was supposed to be giving the seminar, because I can't think of any other reason why someone would be that unprepared. The second seminar leader was considerably better. Our POD (oops, I mean ARM) talk today was a basic science one about several proteins involved in the vasculitis immune response. I was initially feeling wary of an entire hour-long talk that was chock-full of pictures of gels and immunoprecipitations, but it actually turned out to be pretty interesting. The speaker had given one of the POD seminars last year too, and this one was completely different.
In the evening, I went to the very first meeting of the new CCLCM Book Club. We had read "Better" by Atul Gawande. I was feeling really tired and cranky, and I almost didn't go. But in the end, I'm glad that I did go, because it was a lot of fun. One of the things that I liked best about it is that we had a mix of first, second, and third years. I had never thought about this, but having people from different classes meet to discuss ethical issues is a really great way to get a lot of different perspectives. I don't think it would work so well for PBL, but it might be useful to have some mixed-class FCM small group discussions.
Subscribe to:
Posts (Atom)



{kind=link}
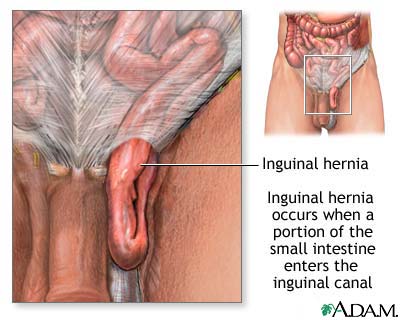{kind=link}